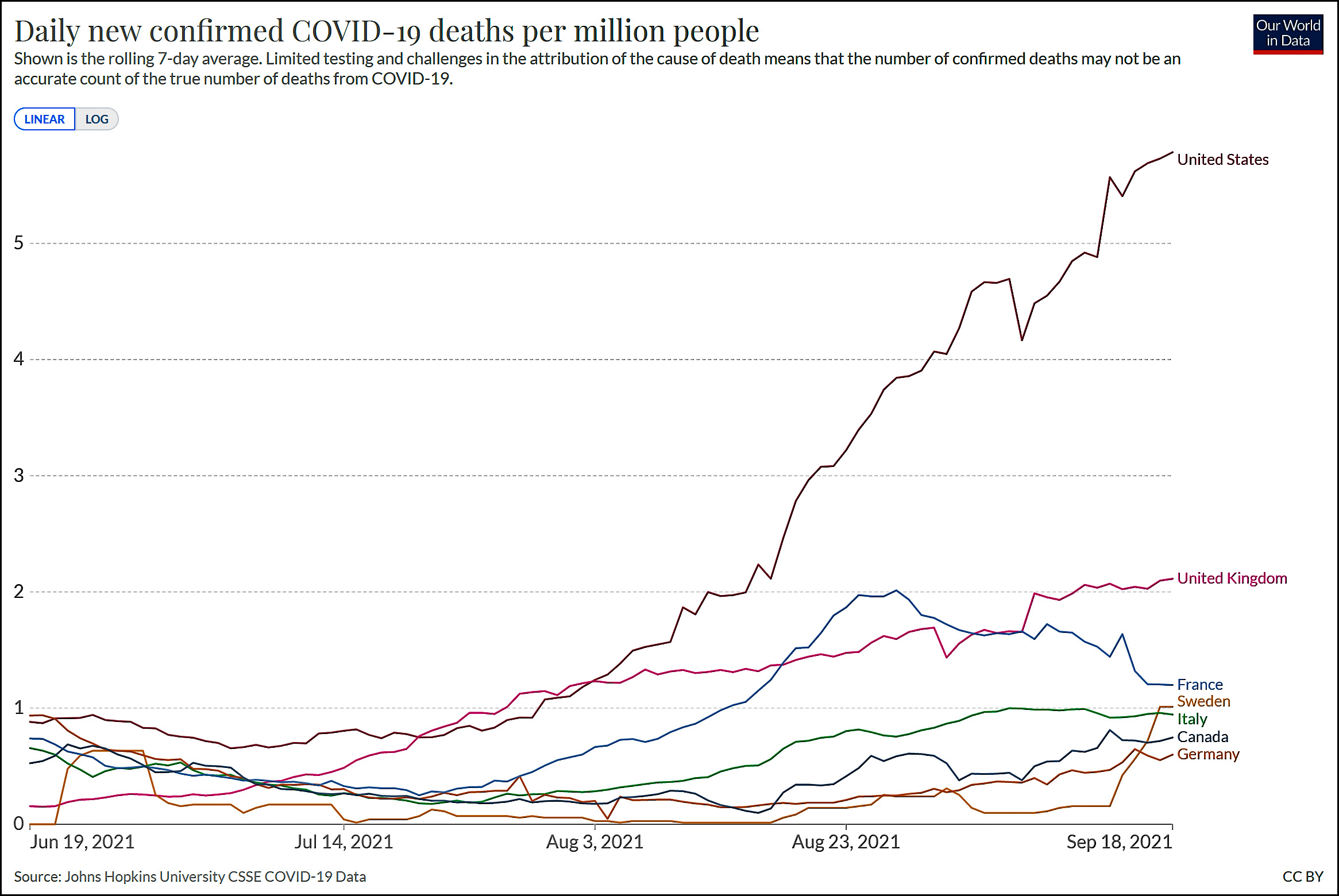
It looks like our mortality rate from COVID-19 is starting to reach its peak. Maybe. I guess that's good news, though this chart is frankly too depressing to think that anything in it represents good news.
Cats, charts, and politics
It looks like our mortality rate from COVID-19 is starting to reach its peak. Maybe. I guess that's good news, though this chart is frankly too depressing to think that anything in it represents good news.
Comments are closed.
God news, everyone!
SARS-like viruses may jump from animals to people hundreds of thousands of times a year,
https://www.science.org/content/article/sars-viruses-may-jump-animals-people-hundreds-thousands-times-year
Accompanied by a lovely photograph of a bat flying straight down someone's throat.
Also, good news.
Finally a reason criminals are afraid of bats. So I suppose they are afraid Batman will give them a killer flu.
Infectious Lass, she can give any guy a disease,
https://comicvine.gamespot.com/infectious-lass/4005-47108/
I’m definitely not a chart person but could someone please explain why Kevin thinks this chart indicates that domestic Covid-19 deaths are peaking?
Because if you imagine a trend line with your Mk I eyeballs it suggests the rate of increase is decreasing which itself suggests, perhaps in a Pollyanna way, approaching a peak.
Best indicator is hospitalization. Once that peaks, almost surely deaths are peaking a week or two later. Hospitalization is the hardest most current statistic.
Looking further down the road, you can see a little further into predicted future with case numbers but they are more subject to distortions from holidays , testing levels etc. . But that looks to have peaked a few weeks ago.
Note that both cases and especially deaths are still affected by holiday distorting numbers. Labor day is finally unwinding. Looking at 7 day averages, the week which includes labor day and day following will show a trend down a bit which is not reality and opposite for week following when the trend will look too high by a higher margin ( comparing numbers too high from labor day catch up to numbers too low from missing labor day #s), then a trend bias a bit too low ( as normal compared to too high).
Adjusting for that, looks more like we peaked and maybe are declining a bit now. But holidays are messy. And largest county Los Angeles took the weekend following labor day off for readjustment and then reported three days at once last Monday. Some did not adjust for that and it screwed up the averages. Clearly covidactnow did not adjust for that showing too high #s for a week and will drop tomorrow.
Also not sure what different reporting sites are doing with fla reporting and any other states that report based on date of death. As I have said , you can always still get the old way and use number based on reoort date but some ( worldometers) clearly is not. Lumping in as one national number different state figures reported different ways does not work.
The way fla is reporting is superior and reality. If everyone did that, you would always see a dip in last few weeks as those numbers are incomplete and still being filled in. Which then means, which is true , that we just do not know yet what actual deaths are for recent weeks. Showing deaths by date reported has misled as to what we know. Plus distortions affect that. Once you have the deaths by date of death , that is showing real trends .
Note , now that we can sew old deaths by date of death, it is clear that the peaks and troughs are more extreme than by report date .
Can’t speak for Kevin but looking at Worldometers it appears that new cases went down last week and deaths went down a bit too.
It used to be depressing, but not anymore.
An anti-vaxxer mother and her daughter died just days apart in a Belfast hospital after they contracted Covid-19, leaving their family “devastated”.
The BBC reported that Sammie-Jo Forde, 32, died in the Ulster hospital on Saturday, where she had been treated on the same ward as her mother, Heather Maddern, 55, who died on 31 August.
To the extent this sort of thing is happening all over the world, we’re all better off in the long run. Silver linings.
Occasionally, though, some foolish people get caught in the COVID crossfire. But even this is some sort of lesson for the foolish. Unvaccinated because... too foolish or something.
https://www.freep.com/story/news/local/michigan/2021/09/19/detroit-couple-died-within-hours-each-other-covid-19/8346378002/
What is there left to say about this stuff? Nothing.
Not forgetting that GQP States ALWAYS show *low* mortality rates .
No they don't. Are you just jumping to a conclusion you want to believe or looking at data .
Assuming you are talking about case fatality rate , that is influenced by a number of factors.
1) testing levels. The more testing, especially random testing, the lower case fatality rate , of course . Almost all deaths with covid are being picked up so biggest issue is how many cases with no or few symptoms are being found.
Here currently gop states tend to test less which makes their cfr higher than blue states. But there are exceptions with both red states with high testing and blue states with low.
And low testing availability was most prevalent in first wave and largely resolved by fall 20. Since then testing differences are policy not availability. The states that had a huge early wave like ny and NJ missed a large percentage of cases then ( some deaths too but not near as high a %age) .
2) first wave in NY nj and some other places overwhelmed health care and some medical treatments like overuse of ventilators turned out to be a bad idea. So early states had higher cfr.
3) the stupid nursing home policies in NY, NJ, mi, CA were a factor early on increasing deaths in these generally blue states.
4) in latest wave , more vaccinations, higher percentage of cases are breakthrough so lower current.
Note blue states are still higher in cumulative cfr as the factors in #2, #3 and #1 for first wave still are biggest issue for cumulative cfr in states like NY.
Aha. Now we know WHY the Israeli study and the UK study vary so wildly in their assessment of vaccine Immunity(VI) versus Natural Immunity (NI). The Israeli study said NI was slightly better than VI under their test. The UK study said VI was better than NI in theirs.
Keep in mind the Israel is using the Pfizer vaccine almost to the exclusion of all others whereas the UK is using Pfizer, Moderna and J&J.
https://www.post-gazette.com/news/health/2021/09/18/Big-gap-between-Pfizer-Moderna-vaccines-seen-for-preventing-COVID-19-hospitalizations/stories/202109180045
{snip}
Data collected from 18 states between March and August suggest the Pfizer-BioNTech vaccine reduces the risk of being hospitalized with COVID-19 by 91% in the first four months after receiving the second dose. Beyond 120 days, however, that vaccine efficacy drops to 77%.
Meanwhile, Moderna’s vaccine was 93% effective at reducing the short-term risk of COVID-19 hospitalization and remained 92% effective after 120 days.
Overall, 54% of fully vaccinated Americans have been immunized with the Pfizer shot.
{snip}
So, once the data gets scrutinized it appears as though Pfizers VI wanes much faster that the others. How badly?
{snip}
Once the Moderna and Pfizer vaccines were rolled out to the public, their records of preventing COVID-19 hospitalizations in the first four months were neck and neck — 93% and 91% effective, respectively. But the degree of protection diverged after that.
When they focused specifically on the period 120 days beyond the second dose, the study authors found that the Moderna vaccine remained 92% effective at preventing COVID-19 hospitalizations. But the equivalent figure for the Pfizer vaccine was 77%.
{snip}
When compared in an equal basis the Pfizer vaccine is WORSE than the others after 120 days, 4 months. But Pfizer is insisting its good. I get the argument but now that the Israelis are rolling out 3rd shots and prepping their population for 4th shots. This seems to be an economic boom to Pfizer. Meanwhile is the way the shots are administered? Moderna is 4 weeks between first and second shot. Pfizer is two weeks. That argument is also made by herd immunity folks.
The answer is no - not by a long shot:
{shot}
Both the Pfizer and Moderna vaccines are based on mRNA technology, which delivers temporary instructions to the body’s muscle cells that help it learn to recognize the spike protein, a key part of the coronavirus’ structure. But “they’re actually not necessarily interchangeable,” said Dr. Timothy Brewer, a professor of medicine and epidemiology at UCLA.
Each vaccine is formulated and administered differently, Brewer said, and those differences could affect the strength and duration of the two vaccines’ protection.
Moderna’s shot contains 100 micrograms of vaccine, more than three times the 30 micrograms in the Pfizer shot. And Pfizer’s two doses are given three weeks apart, while Moderna’s two-shot regimen is administered with a four-week gap.
Brewer also pointed to evidence that the Moderna vaccine seemed to elicit higher levels of a key antibody than the Pfizer vaccine.
{snip}
If this information is correct, and it is the second article I have read on this since the FDA denied authorization for 3 shots here in the U.S. - then it completely undermines the Israeli study's results
They compared a weaker vaccine with less antibody generating capacity against NI and came to the erroneous conclusion that VI was at best equal to or just slightly less than NI over time.
This is false. Pfizers vaccine is weaker and does not elicit the same anti body reaction the others do. It is weaker - MUCH weaker than the others and happens to be administered over a 4 week interval.
The UK study found VI to be better than NI - but their results are skewed to the weaker side because they INCLUDED PFizer in their study.
When you stick with Moderna and J&J vaccines you get far better protection because is stronger
Enough with the NI argument already. Yes you do get NI and yes that is a good thing but you have to get sick to get it which is bad, VERY bad. All the vaccines work - ONE is much weaker than the others. To include that in the studies is weakening the results.
And this is not unusual when it comes to vaccines. Two years ago I was at a routine physical and inquired about my annual flu shot. The Doc said: "Mr Vog - get you flu shot at Walgreens their version is 25% stronger than the one I am administering here in the office. With your health conditions I'd feel better if you got the stronger shot this year."
Ah, I always suspected the claims of "Natural Immunity" were based upon a foundation of sand. My entire local family got the Pfizer shots, so I guess we'll all have to be careful to avoid breakthrough cases.
And the Moderna first shot alone was much better than the Pfizer first shot--close to the the J&J single shot results. Kevin mentioned a dose response study months ago--which was very interesting.
One correction, the UK mainly used the Oxford-AstraZeneca vaccine. Same type of vaccine as the J&J, but administered in two doses. The UK also had a first dose first policy, so longer times between first and second shots. First dose effective enough against original version of the corona virus, not so much for variants.
Rumor has it that Moderna vaccine is not tolerated as well, i.e. you're more likely to get a fever the next day or so. The Pfizer vaccine has issues with myocarditis--I think Moderna has similar side effect, but not so much for J&J which has other issues:
https://www.theguardian.com/world/2021/sep/10/boys-more-at-risk-from-pfizer-jab-side-effect-than-covid-suggests-study
Pfizer has done a much better job at science by press release. You don't hear much from Moderna and J&J has had some problems.
golack-
"Rumor has it that Moderna vaccine is not tolerated as well, i.e. you're more likely to get a fever the next day or so"
So the Moderna vaccine is 3X stronger than Pfizers so yes, side affects are probably going to be 3X mores serious but in this case were not.
Pfizers vaccine just like all others will work better when "boosted". All vaccines do. It's a question of when to administer the vaccine. It looks like with the Moderna shots you get stronger protection for longer periods of time. So for the Moderna users you have to take boosters at a longer interval.
But the Pfizer weakness at 4 months explains EVERYTHING the Israelis are doing with 3rd and potentially 4th rounds of shots.
It also explains why Pfizer's vaccine may be more applicable to younger children because of it's "weakness"
NI arguments are slowly going by the wayside as more information comes out.
Didn't the UK delay second shots by weeks or months anyway?
The UK did indeed delay the second shot of the Astro-Zeneca vaccine when they had reports of severe reaction to that vaccine.
Most of Canada followed a policy of getting as many first shots as possible administered as quickly as possible, and so delayed second shots, with intervals from eight to twelve weeks between first and second shots. It would seem there should be some useful data there about the effect of longer intervals between shots.
Any chart that tracks the impact of Conservatism in America is depressing....
For those curious about the sudden upturn of the Swedish curve: Death numbers are rising in Sweden, but not as steeply as it seems in this chart. As I mentioned a couple of weeks ago, there were major system updates to the death registry which prevented death reporting for some time, with subsequent catching up.
For a more accurate picture of covid deaths in Sweden, please see
https://adamaltmejd.se/covid/
where deaths are shown on the actual death date, not the date it was reported. In Sweden covid casualty is defined by death occurring within 30 days of positive diagnosis.
I had not seen the Swedish criteria of counting if within 30 days of positive test. I think most of usa and uk has been going with a 60 day rule and so is more expsnsive . Which would mean that, in comparison with usa and uk, Swedish deaths are biased a bit low.
The data showing reporting delay does show the delay being longer at peak times . Any delay itself will tend to slightly flatten the curve ( reduce the height of the peak and the bottom of the trough) if you look at reporting date and the change in delay will accentuate that and also make the peak look too late even adjusting for delay.
As far as I understand at least the UK use death within 28 days of COVID diagnosis.
It is frustrating because you cannot find good info on the criteria in the USA which seems to vary depending on place and time . I thought I had heard that the cdc standard was a positive test within 2 months but looking again I am just confused as to what is being done.
And first glance it seems that red states are often using a more expensive definition than many blue states which goes against expectations.
Personally I would rather a simple objective criteria like any death within 60 days of positive test - at least for counting total deaths. Yes, that means for example counting George floyd as a covid death or someone in an auto accident.
This is only for cumulative numbers because then you can adjust put reasonably for expected number who would die anyway without covid ( i.e. subtract out those who die normally in 2 months). To be able to make that statistical adjustment, you cannot exclude anyone from start .
I know many use " excess deaths " as an estimate but that is seriously flawed. First, of course it does not take into account the unknown extra people who died due to other things changed, especially covid restrictions ( loneliness, depression, job loss, breathing issues and infections from masks, etc. ).
But also, in usa, the baseline usually used of average deaths from 15 to 19 is biased too low making excess deaths likely higher than they really were.
Vog,
Saying that the Israeli study is " completely undermined " is ludicrous. Clearly, if Israeli almost exclusively used phizer , the Israeli study could only be comparing natural immunity to phizer vaccine immunity. They were not claiming anything re some vaccine that they were not measuring.
And , given the time of the study and vaccine rollout , they would not have much info at that time re vaccine effectiveness after 120 days . By what it had to look at , it could only be measuring effectively phizer vaccine immunity for under 120 days, when the cdc data shows it to be pretty good. And compared to both similar term natural immunity and longer term natural immunity.
If it found that natural immunity was far better then phizer vaccine immunity, this was NOT mostly due to phizer immunity waning after 120 days as most of their vaccine data was before that.
If anything, this would reinforce their conclusion. If phizer vaccine immunity within 120 days really is similar to Moderna immunity either before or after 120 days, then natural immunity would be still better than Moderna immunity - i.e. roughly the same as what the study found for phizer shorter term vaccine immunity
"And , given the time of the study and vaccine rollout , they would not have much info at that time re vaccine effectiveness after 120 days"
The statement above is wrong. As of March 12 Pfizer was }ALREADY releasing information on its effectiveness against the more infectious UK variant
https://www.ajmc.com/view/a-timeline-of-covid-19-vaccine-developments-in-2021
From Feb 26:
"Israel Reaches a Vaccination Milestone
Israel becomes the first country to have vaccinated half of its population, a major milestone on the road to herd immunity, Bloomberg reports. The overall rate of infection slows, as does the rate of critically ill COVID-19 patients in hospitals. Nearly 3.3 million people have received 2 doses of the Pfizer/BioNTech vaccine.
There have been many trials and many roll outs. but by the first quarter of THIS YEAR 4/1 - 50 million doses had been administered just here in the united States.
Israel has had PLENTY of time to study this and the world has studied the others
Do you actually think of what you are saying before you post?
The issue is phizer vaccine effectiveness declining after 120 days from a week after 2nd shot , right?
So that only matters AFTER 120 days from the week after 2nd shot which should be roughly a month after 1st shot so four months or so after 1st shot .
Israel started vaccination 12/19/20. The first group would only have reached the post 120 day period about mid or late April. Basically the entire Israeli study was looking at phizer vaccine effectiveness within the first 120 days when the phizer vaccine is strong just about same as Moderna per that cdc info.
And you then quote a lot of things from well within the 120 day period to disprove it?
Just stop a minute and take a breath and actually read what I said and think and you have to see it.
No think about what the original point here was and that is when to give a booster shot
No one is arguing the need for boosters at 120 days because MOST vaccines are effective at that point.
its what happens AFTER 120 days that IS IMPORTANT and this is where PFizer falls on its face to which the Israelis are REACTING to by pushing 3rd and 4th shots already
So after 120 days? 4 months
150 days = 5 months
180 days 6 months?
Whens the best time
Apparently it depends upon your vaccine type because Moderna is showing far less loss of protection as it pertains to measuring as to when its best to give a booster
Vog,
You refer in 3 different places in your post to the gap between 1st and 2nd dose of phizer as 2, 3 or 4 weeks. I think the standard everywhere in is was 3 weeks. Not sure if you had a point re different number or just made a mistake when you said 2 or 4.
And note that , here is usa, if comparing phizer and Moderna, we really are comparing phizer with a 3 week gap with Moderna with 4 week gap ( not sure re Moderna but you did consistently say 4 there so assume you are right) . Seems clearer at least for phizer that our 3 week gap was too low - maybe just an extra week would have helped. The nation's that did get all 1st shots first and a bigger gap do seem to have done better.
Vog,
You never did respond when I questioned your disagreement with me when I said it seemed clear that vaccination does improve natural immunity and you referred to some uk study that disproves that .
Can I now just assume that you incorrectly read my post and were responding to what you thought I said ( but did not ) and not what I actually said ?
Clearly if you believe that vaccine immunity alone is better than natural, it has to improve on natural immunity too ( even if all that did was supplant natural).
I had COVID
60 days later I started teh 2 shot Moderna regime I had a anti body over load which I stated at that time.
I can no longer tell if the VI is better than the NI in me because MIXING the two lurs the protections line
The CDC measured the protection provided from the date of the FULL vaccination. If it was one shot then it was frfom the date of that shot'If it was a two shot dose it was from the date of the second shot. 120 days. Period. The Israeli study measured the same way and found protection waning from the date of the last shot.
In order to test correctly the studies have to keep the information standard.
They test for people who had one shot of the two shot regime.
Let me \make this simple for you
Pfizer is the weaker of the vaccines. It has a different make up than Moderna does as the CDC alluded to
Pfizer;s weakness over time therefore makes NI look better than it actually is
I did not go overboard twisting words, making assumptions and generally trying to make the argument FOR NI over VI - you did. And you still are.
The Israeli study - and its conclusions that NI is slightly higher than VI is therefore based upon the weakest vaccine and way off base - which explains the 3rd and potentially 4th round of shots the Israelis are pushing.
Sorry but your "political slip" is showing
Pfizer will probably get approved for children first as its the weaker of the vaccines. As my story snips alluded to Moderna not only protected for a longer period of time - "Brewer also pointed to evidence that the Moderna vaccine seemed to elicit higher levels of a key antibody than the Pfizer vaccine"
Just admit you are a herd immunity person and be done with it
Vog,
Really it is you who are just totally insistent on making non existent points to presumably support your political position.
So you just completely ignore the point.
So let me go through this again simply so maybe you can understand ( or more likely be willing to do so as have little doubt you are intelligent enough)
The Israeli study looked at vaccine effectiveness in the first four months after the vaccine ( starting one week after 2nd dose) . THEY WERE ONLY LOOKING AT FIRST 120 DAYS or maybe a day or two more. How much phizer vaccine might weaken AFTER 120 days is completely irrelevant to the study results.
You seem to want to say that the result showing that natural immunity was better was only because phizer vaccine is not so good because it wanes after 120 days . But they were looking at first 120 days when phizer vaccine is still strong per that cdc info .
So your point is simply 100% indisputably incorrect.
See my post above
The 120 day period IS important in the discussion as to when to give a booster
After 4 months (120 days)
After 5 months (150 days)
Or after 6 months (180 days)
Pfizer needs a booster after 120 days as its protection weakens substantially.
THAT is what the discussion is about
Let me throw out one thing I saw in the Bangladeshi mask study in the cost benefit part . It said surgical masks were more effective than cloth, of course.
But also said that cloth masks cost MORE than surgical.
Is this true ?
If so, why is anyone using cloth?
Cloth masks tend to be prettier.
That said, I have some KN95's with tie die and galactic designs.
Is it really that some are valuing fashion over both safety and cost?
If so, that is depressing.
I thought maybe it was that cloth masks cost more but can be washed and reused more than surgical masks so cost per use is less.
If some are using cloths masks to save money even if not as effective, that seems believable. But that study said surgical masks cost less per use .
N95 masks are what I wear. But I live alone and , do to medical issues, cannot be going out to indoor places for long times anyway. And I can reuse the n95 mask a number of times if my use per time is short and let it sit in sun .
If I had to work in a grocery store wearing a mask 8 hours a day, I could see how difficult it would be to wear an n95 mask , both in cost and comfort.
I could deal with cost. But now as I am able to do things a bit more and am out sometimes wearing a mask for over an hour at a time, I am finding the n95 masks just real uncomfortable and they give me headaches and jaw aches.
The cheaper Chinese made n95 masks are not as uncomfortable but also clearly not as effective as usa made . I could tell when there was smoke in the air from forest fires. Cloth masks you could smell the smoke right through them. Surgical a bit better but not great. The Chinese n95 occasionally a whiff of smoke. The USA n95, not one scent of smoke.
Does anyone know an effective yet comfortable n95?
If memory serves me correctly the Bangladeshi study was done BEFORE Delta took off
In the case of Delta a cloth mask is better than no mask at all.
And weren't these folks rural villagers rather than urban dwellers? With most activity taking place out doors?
Not sure of all that ( especially the outdoors part ) but does not matter as to what I was discussing.
Which is that it said in the cost effectiveness study that surgical masks are cheaper to use than cloth. Note not just more cost effective - i.e. cheaper compared to how effective they are , but just plain cheaper.
So what variant, where, etc. Is irrelevant on that point.
Since I only bought two cloth masks ( in April after vaccination when I had hoped i might be optimistic enough to just use them - that lasted a week) and no surgical masks, I just do not personally know the costs.
Sure it matters as to which population center you use.
With delta the Urban centers are where people are closer together and with viral load imposed by Delta is very much different then alpha or beta
From the study:
" The preprint paper, which tracked more than 340,000 adults across 600 villages in rural Bangladesh, is by far the largest randomized study on the effectiveness of masks at limiting the spread of coronavirus infections."
Rural Bangladesh?
Before Delta?
It does not matter for the COST of masks and that was the only thing I was talking about here re Bangladesh study . It had nothing to do with the study or Bangladesh itself, it just happened to be that the study used it to determine the cost side in a cost benefit analysis.
I could also have criticized that analysis logic as it ignored many types of other costs but all I was talking about was cost of masks.
I would guess you do not know personally maybe either as you have used n95 only too?
Last year, death rates in the U.S. hit a local minima around October 8th. In another two or three weeks, death rates might be likely to rise again.
On the other hand, reportedly around 500K people have been infected per day. 15M/month. Give or take, that's about 50% of the population in the past year. Coincidentally, 50% of the population has been vaccinated. So we might finally be approaching herd immunity.
The problem is not with your math
The problem is we don't know who has been sick because? We didn't test.
We encouraged but nobody wanted to know. Our leaders during the stages didn't want to know because they thought it would make them look weak.
Now we don't want to know because the pharma companies don't want to look like they're putting out a weak product.
If you are a documented vaccine recipient and you test positive its a breakthrough case. Bad for big pharma
If you had it before and you get sick its bad for the anti vaxxers because it show NI is weak as well.
And for those that have had COVID - knowingly or not - once YOU get vaccinated scientists cannot determine if your NI is enhanced, or your VI is enhanced because once the vaccine or the virus is in you your body REACTS to it, which differs for each individual. For vaccines the reaction is more consistent (which is why it's universally accepted that everyone should get vaccinated).
We, as a nation, have acted terribly to this virus. We allowed for politics to drive science. WE didn't test enough. We downplayed the virus. We attempted bizarre and dangerous treatments. But because we are spoiled we didn't want ANYTHING to interfere with our lives. Masks? Social distancing? Bar and restaurant closures? All bad. All an affront to our freedoms.
When Delta came around we were not prepared and we paid a price.
Now since we didn't do what we NEEDED to do up front? WE have to rely on foreign countries for more complete data. And that is not good. Israel chose the wrong vaccine which weakened far too quickly. They are now talking about 3rd and 4th doses. Here in the U.S. we are using every excuse to NOT have to get a shot or wear a mask,
And now, as insurers are getting involved, and co-pays become more common place for COVID testing, and treatment, even fewer Americans will attempt to mitigate this global calamity.
And with Flu season starting up? More children being affected by CV Delta? it's going to be a rough winter
You can measure vaccine efficiency and NOT have to disclose that you had or didn't have COVID.
Get the shots. Wear your masks. Or pay for continued testing and/or lose your job if you have to deal with the public. Someone OTHER than you could pay the ultimate price.
You are not just saying add 50% to 50% and you get 100%, are you? It is not nearly that simple.
First you have to define what you mean by " herd immunity " . The concept is that, once enough have some immunity, the virus will not effectively spread, so that even someone with no immunity is effectively protected by the "herd" with immunity as there is too little virus around to be infected.
Basically, if R is below 1.0, you have reached what you need for herd immunity, if you can keep it there. Even with starting cases high, if R stays below 1.0, they will dwindle away and the risk to those with no immunity becomes minute .
Today, it looks like R is below 1.0 and cases are falling. So based on what you need for herd immunity , we are now there . But we have gotten there before three times already, after wave 1 in spring 2020, after wave 2 in fall 20 and after wave 3 in spring 21. I might eliminate to some extent one of them . First wave really hit northeast hard and spread to rest of nation. Northeast got to herd immunity in spring 20 and basically stayed there till wave 3. Rest of nation wave 2 was really just wave 1 hitting them. So maybe two prior times reached herd immunity but different times different places.
But we did not keep herd immunity any prior time. Reasons were
A) new variants hitting in fall 20 ( alpha and related ) and spring 21 ( delta) changing the base R
B) weather clearly played a big role in fall to winter 20 , especially in North. In South Summer may be worse than winter. For this delta wave, weather most places in North offer delta impact rather than accentuating like with alpha ( so far).
C) waning immunity from prior infections or vaccinations. In fall 20, obviously that would be all natural but comparison of places does not seem to make that a big factor ( would have made ny and NJ worse if it was a big factor) .
Now of course we have to worry also about waning vaccine immunity.
D) maybe lessening restrictions played a role but does not seem major
E) all of that is offset by increasing immunity from new infections and vaccines . If relying solely on new infections to offer waning natural immunity to keep R below 1.0, never really can get to low case numbers. But we do not yet know how good natural immunity is long term.
Will we have another winter wave, assuming R is below 1.0 now. How would we expect R to change.
As old immunity wanes , R increases. But new infections decrease R by increasing immunity. Outside of weather or vaccines, that has to balance to keep R from changing. But , if long term R from natural immunity is good enough, and you overshoot herd immunity as always due to trailing cases , possible long term R can stay below 1.0 and virus almost goes away permanently. But rare and no reason to expect it with covid .
So the question is whether we can supplement natural immunity by continually adding immunity through vaccination ( new or booster) to offset waning immunity and keep R below 1.0.
I expect the answer is no for all seasons but enough to have small waves each winter and then largely going away in spring. Like the flu.
RT
n95s in my area were nowhere to be found
I also have COPD which the Doc said was enough to get me a medical exemption to mask wearing
But I already purchased some filtering masks, Once I had covid and got vaccinated I switched to cloth masks washed daily over a filtring mask, which is where I stand today
Nobody wants to fit test themselves for the n-95s which makes them virtually useless to everyone anyway
I can't tell you how many people I have seen with N95s that also have beards !!!
This is why vaccines are the answer.
If you are dumb enough to NOT follow manufacturers guidelines for a mask, then you are not smart enough to get tested if you feel ill to see if you at least have natural immunity.
Because of all the uncertainly. The changing virus being the biggest factor - herd immunity is a myth in a population that is NOT college educated, doesn't want to get tested or get jabbed and doesn't give a damn about anyone else but themselves.
We WILL see more variants because of our own stupidity. Lambda and Mu even though they may not be taking over yet - by their very own formation during the Delta wave - indicate that UNLESS we convince people to get vaccinated regardless of political beliefs we will NEVER reach herd immunity because the virus WILL mutate.
Vog,
Personal advice if you will take it the right way.
You already had covid . Do you mean you just got tested positive but had no or few symptoms. Or did you clearly get covid symptoms and have a serious illness ( even if not at hospitalization level)?
If you actually became ill with covid , you almost certainly developed good natural immunity. And then you got vaccinated too !! So you have double immunity and that is really quite damn good. You are about as safe as possible.
And you have copd so not great medically to restrict your breathing.
Given your extremely low chance of getting infected and being infectious, you pose a miniscule risk to others. And the masks you are wearing really do not that much anyway. The health risk of restricting your breathing by masks outweighs easily the small protection the masks you wear give you from your already extremely low risk personally of getting covid again .
You have done already two big things reducing your covid personal risk and risk to others. That is getting sick from covid and getting vaccinated too. And have a medical condition making masks risky .
If anyone in the USA is entitled to not have to wear a mask, it is you.
But, as I guess you will still insist, how about trying to find an n95 mask with a respirator. Ask your doctor if that will work for you.
They are available now online I think. Try Amazon maybe. Or maybe your doctor would know.
Here in Los Angeles , n95 masks are available but easier to find in a medical supply store rather than a chain drugstore. But they are in my local walgreens too.
With copd, I would think a normal n95 might restrict your breathing too much . More than cloth masks.
What a respirator does is it allows you to breath out normally so makes it much easier to breathe. Because of that, it is doing next to nothing to protect others but you have done enough there.
rt
No - cloth masks are easier to breathe through. Couple that with a filtering mask underneath and that works for me
My last shot of Moderna was in March. I'm already 6 months out
I will NOT take the chance of catching a break though case
And yes, I know I had the highest level of immunity protection back when I got the second shot they told me exactly what would happen - they called it anti-body over load then.
Sorry but 6 months out is a long time and I have no idea where my protection level is right now. I assume the worst because thats how I operate.
And no, I will NOT wear a respirator. I did that for 20 years when I needed to when I worked for state government.
But very much like COVID. When you know you need to wear one it's already too late
Here's the other reason I still mask up :
https://www.wsaz.com/2021/09/21/cdc-study-says-covid-19-can-spread-vaccinated/
A new study of Texas prison inmates provides more evidence that coronavirus can spread even in groups where most people are vaccinated.
A COVID-19 outbreak at a federal prison in July and August infected 172 male inmates in two prison housing units, according to a Centers for Disease Control and Prevention report released Tuesday.
About 80% of the inmates in the units had been vaccinated. More than 90% of the unvaccinated inmates wound up being infected, as did 70% of the fully vaccinated prisoners.
Severe illness, however, was more common among the unvaccinated. The hospitalization rate was almost 10 times higher for them compared with those who got the shots.
It echoes research into a July outbreak in Provincetown, Massachusetts, where several hundred people were infected -- about three-quarters of whom were fully vaccinated.
Such reports have prompted a renewed push by health officials for even vaccinated people to wear masks and take other precautions. They believe the delta variant, a version of coronavirus that spreads more easily, and possibly waning immunity may be playing a role.
The authors did not identify the prison, but media reports in July detailed a similar-sized outbreak at the federal prison in Texarkana
*******************************************************
We don't know if this is a function of Delta or CV in general.
If we are seeing MORE of this, and so far its been studied in the close confines of this prison AND in the tourist area of Provincetown MA then immunity, in the form of VI or NI may be seriously over estimated as to its efficiency in stopping the spread. Reduce the seriousness, yes, but stopping the spread may be something else entirely
And yet ANOTHER reason why I still mask up even with inefficient masks
https://deadline.com/2021/09/r-1-new-covid-variant-u-s-japan-1234841685/
{snip}
While the Delta variant’s dominance in the United States is nearly universal, news of another spreading strain of Covid-19 has recently surfaced.
Known as R.1, the new variant was first found stateside in Kentucky which, according to Governor Andy Beshear, is among the three states with the highest infection rates. R.1 was first identified via an outbreak at a skilled nursing facility there.
According to a CDC report, among 83 residents and 116 healthcare workers, 26 residents and 20 workers tested positive for Covid. Twenty eight specimens were subjected to whole genome sequencing and, on March 1, found to have mutations that aligned with the R.1 lineage. (The outbreak reportedly began with an infected staffer.) “Attack rates were three to four times as high among unvaccinated residents and [workers] as among those who were vaccinated,” according to the findings.
{snip}
Now - think about the numbers
46 samples were taken - 26 genome sequenced - and were found to have the R1 variant. That is high for a new variant
Now this:
{snip}
Roughly 90% of the facility’s residents and and 52% of the staff had received 2 vaccine doses. Among those, 25.4% of the residents and 7.1% of the workers were infected. That, according the CDC analyses, raises concerns about reduced protective immunity to R.1 from vaccines.
What’s more, four possible reinfections were identified, “providing some evidence of limited or waning natural immunity to this variant,” per the report. All of those people experienced symptomatic illness. One of them died
{snip}
It is not a case of vaccines and masking PREVENT the spread
Apparently they don't do near as good a job than advertised.
Its also not the fact that R1 is going to become dominant
Its the fact that the mutations are occurring in the first place
And the fact that fully vaccinated people can spread it, that previously ill people can spread it indicates that the mutations are happening far more rapidly with COVID than the normal flu.
We may be looking at a "WalMart" type illness here.
We are seeing far too many cases of variants bypassing WHATEVER protection you want to believe in