The Washington Post has a story today about the demise of ER physicians. It used to be a coveted position for residencies, but now senior doctors are warning against it:
They warn of burnout after covid and patients’ increasing suspicion of doctors. The pay is not as good, they say, especially as hospitals rely more on nurse practitioners and physician assistants to staff emergency departments. And job prospects may be grim, they caution, as emergency medicine residency programs aggressively expanded in recent years.
....Emergency departments are under strain as they become congested with patients waiting for beds, veteran providers quit and violence against the remaining staff grows. These factors are damaging the emergency room’s reputation as an ideal place to learn by caring for a steady stream of patients with a wide range of problems.
Every year, graduating students apply for residencies and are matched with programs that are interested in hiring them. Here's what that looks like for emergency medicine:
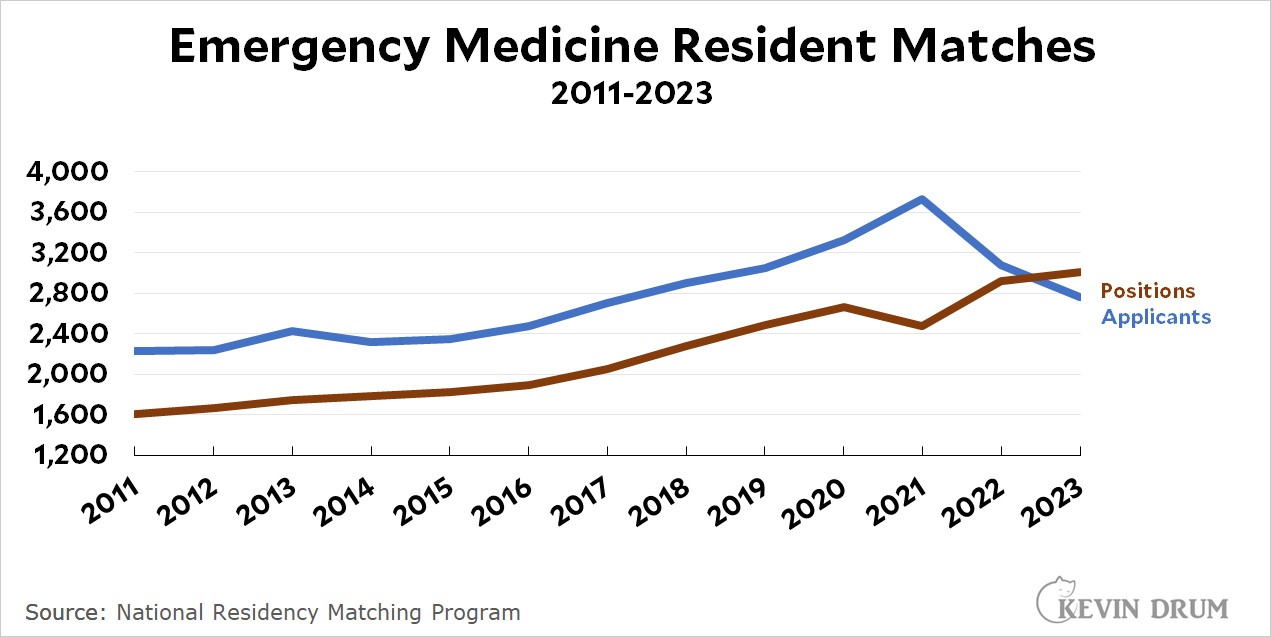 Emergency medicine was in the SOAP in 2023. That is, there weren't enough applicants for all the open positions, which means that some ER residency programs had to hire doctors from the Supplemental Offer and Acceptance Program, a sort of second-round draft for everyone who didn't get an offer from the first round of matching.
Emergency medicine was in the SOAP in 2023. That is, there weren't enough applicants for all the open positions, which means that some ER residency programs had to hire doctors from the Supplemental Offer and Acceptance Program, a sort of second-round draft for everyone who didn't get an offer from the first round of matching.
Of course, it's worth noting that, in the end, every ER position was filled. And every specialty has its ups and downs. Perhaps next year, with ER departments back to semi-normal, we'll see a rebound.
The congested part I understand. My fellow citizens feel that the ED is just a doctor's office. In fact, I have a sneaking suspicion that many in the medical field feel the same way. And the very worst part of a trip to ED (and most likely the source of much of the grievance), is that you probably will be given a pat on the head and instructions to follow up with your physician. You might get lucky with a pain management course. Or not.
Google paid 99 dollars an hour on the internet. Everything I did was basic Οnline w0rk from comfort at hΟme for 5-7 hours per day that I g0t from this office I f0und over the web and they paid me 100 dollars each hour. For more details
visit this article... https://createmaxwealth.blogspot.com
Pingback: Emergency rooms seem to be heading toward trouble | Later On
I know someone who went through matching recently for residency, and I remember them telling me that you could pretty much guarantee a match if you went for ER, general/family medicine, or general surgery. You might end up in some location you hate while doing the residency, but you'll get a spot.
My wife is an ER doc.
Based on what I have learned being an ER doc has lots of challenges.
- high stress
- lots of folks, maybe half, really don't belong in the ER
- EMTALA means hospitals want you to push people out https://www.google.com/search?q=EMTALA+mandate&oq=EMTALA+mandate&aqs=chrome..69i57j0i22i30l3j0i390l2.1310j0j15&sourceid=chrome&ie=UTF-8
- compensation is better in many specialities
- hospital satisfaction scores 'matter' but can be gamed and are semi random
- drug seekers are common. Fake symptoms in search of meds or even, trying to steal meds.
-
Met an ER physician a few years ago on a dive boat vacation. We had the misfortune to have a couple of incidents that required her attention. It was notable that she was clearly an adrenaline junkie who liked being involved in real emergencies. I can see how such a person would find our present policy of using ER’s to distribute normal health care unsatisfying.
I've also responded to my share of emergencies on dive boats, sailboats, and airplanes! I guess I have also been accused of being an adrenaline junkie, but I think it's more just that I spent my entire adult life developing a very specific skill set, and it's nice to be useful. Like a programmer who takes pride in squashing a bug, or a lawyer who spots an inconsistency in a deposition. It looks hard to others, but this is just what we do. Personally I would be happy with a lot less adrenaline in my body. But you are correct about this: if you don't have an immediately life-or-limb-threatening condition, I don't know exactly what your experience will be under my care.
That chart looks like the trend change is due to COVID and concomitant hostility towards the medical profession (mostly by anti-vaccination people).
That was hard, but that's pretty much over now. The big struggle now is lack of labor and beds for the chronically ill, which leads to clogged up hospital beds, which leads to boarding in the ED, which leads to long waits for anyone who is not immediately dying, which leads to severe chronic stress for anyone brave enough to keep working in the ED.
You've identified one of the big problems with health care, and it's a problem not restricted to the US. Health care tends to be "siloed". There's a "doctor's office" silo, a "hospital" silo and an "extended care home" silo, just to name a few, and the sizes of the siloes are often not in proportion to each other. Especially with the population aging, there's a desperate need that never seems to be met for extended care beds. There need to be enough doctors for the number of patients, and enough regular hospital beds and extended care beds to give those doctors places to send patients that need more care than they can be given in the doctor's office. Of course, there also need to be enough trained personnel to properly operate the hospitals and extended care facilities, which brings in at least another two siloes, med schools and nursing schools.
A lot of doctors love working in an ER because it gives them an opportunity to play games with insurance and give patients massive, unexpected bills that are not covered. I wonder if that teach that trick in medical school?
realrobmac - I am bias because my wife is an ER doctor. With that said, based on your statement, you have no idea how billing and doctor compensation works.
Further, while doctors do want to be well compensated given the rigorous path they must overcome, my limited experience is making money seldom sustains an ER doctor's career. Then again, I don't have an un bias perspective....
I know the hours our ED docs work and know their pay. In general their pay is average and in some places probably 30th percentile so low average, but also as a rule their hours are much less than that of others. Their hours are about 60% of what I work. That said, there are some ED docs who do well by not participating with the insurance products that their hospital participates with. However, that is usually the decision of the hospital so they can avoid subsidizing ED salaries.
Talking with the ED staff (their chair and I are good friends) I think covid has left a big hangover. The covid deniers are a pain to deal with but its just one more hassle and not the biggest. I think our ED docs are most perturbed by how often they end up holding pts in the ED. Hospitals try to run lean to keep costs down so that means that in busy times like Flu season and intermittently at other times they cant get people admitted. This is mostly predictable but overstaffing to be prepared would cost a lot. Covid really exposed this even more. The other factors are chronic, like having to act as a substitute PCP, and I dont think have changed much. I actually expect that to be better in a lot fo systems since networks have found out you can make money in urgent centers. Same with the stress, The ED always had some stress (with lots of boredom) and if that has changed a lot fo that is that now you arent doing what you trained to do, see pts and move them along. Most ED docs dont want to be hospitalists.
Steve
And let's not forget the MASSIVE gatekeeping performed by the AMA to ensure that there are always only barely enough doctors available (thus keeping salaries high).
It's pretty inevitable, if you are playing these sorts of games, that every so often you do the accounting slightly incorrectly and generate a glitch in some specialty.
Both the education pipeline and allowing in medical immigrants could easily resolve this issue if it were actually serious.