Assuming I did my sums correctly, here are the death rates for all 50 states plus DC from January 1 to the present:
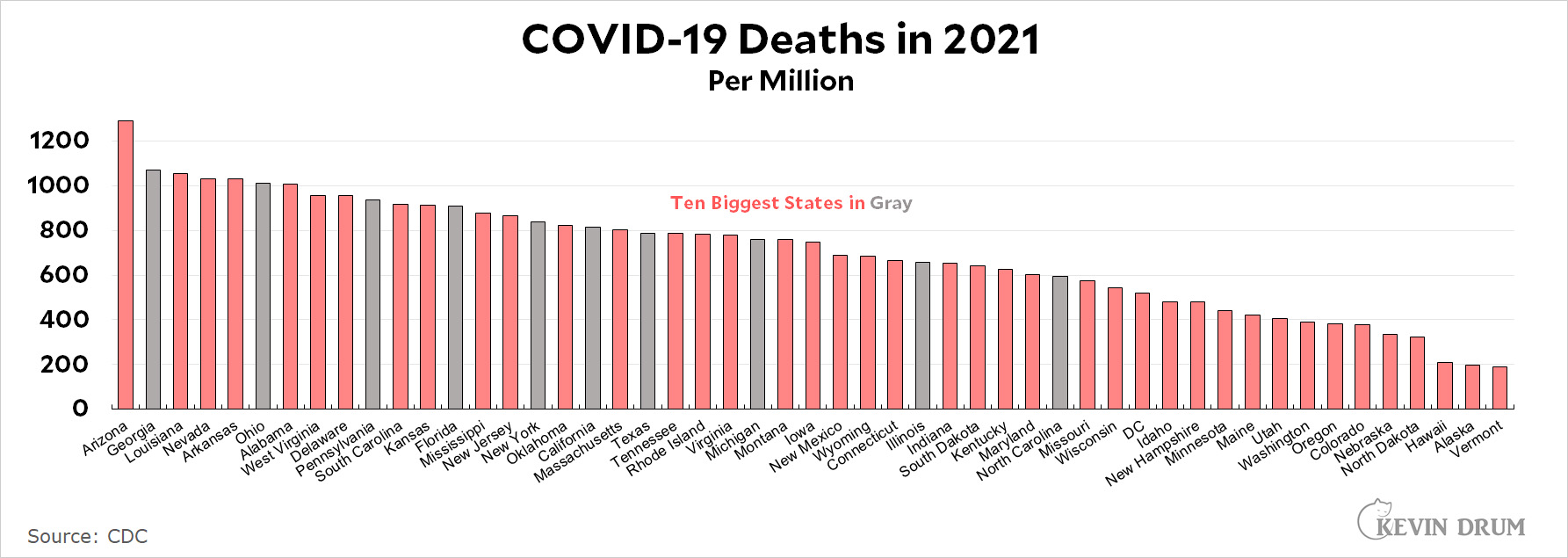
It's small and hard to read. Sorry. But you can right-click to enlarge it if you need to.
Cats, charts, and politics

Assuming I did my sums correctly, here are the death rates for all 50 states plus DC from January 1 to the present:
It's small and hard to read. Sorry. But you can right-click to enlarge it if you need to.
Comments are closed.
I'm a little shocked and surprised that California has a slightly higher death rate than Texassistan. I'm going to have to look at our data by the county level to see what's going on...
https://docs.google.com/spreadsheets/d/1BG_FI49tB4tEqs5c45uEB-fR8WIqz6pHqVv87gXp0gM/edit?usp=sharing if it is of help.
Very nice! I'd been looking for something like this. Where did you get this? (No, doubt some publicly accessible data base that everyone knows about except me.)
Oops. This is cumulative per day. Is there a data source with deaths reported per day per county? It looks like on some days counties adjusted their cumulative totals downward, so I get some negative numbers when I subtract previous day from current day to get the deaths per day. Still lots of great data here!
Anyway...
COVID-19 cumulative deaths (3/1/20-8/27/21) per 100,000 population for the top 16 Most Populous Counties in California (greater than 500K population)
San Franciso 66.3
Contra Costa 75.3
San Mateo 77.6
Alameda 78.5
Santa Clara 92.4
San Diego 116.1
Sacramento 122.4
Ventura 127.7
Kern 162.0
Orange 163.8
Fresno 177.2
Riverside 191.3
San Joaquin 198.5
Stanislaus 205.8
San Bernardino 244.9
Los Angeles 251.2
We can see that SF Bay Area counties did much better than the Southland counties, Inland Empire counties, or Central Valley Counties. Though San Diego, Sacramento, and Ventura County didn't too badly.
I think part of the difference is that the SF Bay Area counties (led by Dr. Sarah Cody, the public health director of Santa Clara County) asked people to start working from home the last week of February 2020, and they were urging masking and social distancing by the first week of March (I remember Dr. Fauci said we were overreacting). We really started our "lockdown" several weeks before Governor Newsom announced a state-wide lockdown on March 19.
And in the SF Bay Area, we've remained heavily masked. I no longer see Karins and Kens and complaining about wearing masks indoors (they just do). And a lot of people are wearing them outdoors. So I think this is why the SF Bay Area has come through pandemic relatively unscathed (so far).
Rick, I think you are incorrect in the differences in sf bay area and Los Angeles.
In many respects early on, la was ahead of the bay area in imposing restrictions by govt. Especially in late spring early summer . The bay area was a bit ahead in asking for voluntary things like you mention. But the la area imposed harsher mandatory restrictions at first. Like actual 10 pm curfews that were being enforced to some degree by police.
Plus the big difference in cumulative is from after the first wave- almost all the second winter wave. And through almost all of the pandemic, la was under harsher govt restrictions than the bay area . Because we had more cases and thus were in a higher state category- plus the county itself sometimes stuck to tougher restrictions than required by the state.
No way does tougher mandatory govt restrictions explain the difference between la and af area because it is la that had the tougher restrictions almost the whole time.
Much more likely is compliance with the restrictions which was higher in the bay area.
And more other differences. La is more Hispanic, especially poor Hispanic. Often living in more crowded conditions with many family members under one roof, which makes it real easy for covid.
Plus look at the economy. The core industry in sf area is high tech. Easy generally to work from home there. La is entertainment. How are you shooting a movie remotely?
But main thing is difference in number, type and concentration of Hispanics. La and sf areas do not differ much in covid looking just at black white and Asian. But they do for Hispanics and la is also more Hispanic.
La Hispanics got devastated in the winter wave. Partly due to conditions and partly because they were the group mostly not complying with restrictions, especially at first. They were not in denial - just valued living life well vs preventing death. I did discuss this with a number and you just could observe noncompliance.
Today I have noticed that Hispanics are complying with masking more than they used to.
From my observation, re racial groups,
A) brazen non compliance like refusing to wear a mask at all where required- more likely white
B) passive noncompliance wearing mask below nose - more likely black
C) minimal compliance- only wear mask when required and never when not - mostly Hispanic
D) always mask no matter what - more Asian
Rational Tought:
When were asked/told to work from home? My company had me working from home the week of Feb 24th 2020 after several suspected cases were reported at various Silicon Valley companies. All the big companies except Lockheed voluntarily complied with this request. That same week London Breed, mayor of San Francisco put out a request the people shelter in place.
When were you told to start masking up? For me it was the week March 2nd 2020. There was a shortage of all sorts of masks and hand sanitizers at that time. But various county and municipal websites started putting up "how to make your own mask" instructions. And the message was that any face covering was better than nothing.
First week of March, San Francisco was a ghost town. All he freeways were empty at rush hour.
Was that the case in Los Angeles?
I start with the same Johns Hopkins data as Kevin. There is a tab in that sheet for per dap per million over the last seven days. Need to use trailing averages.
The big picture:
https://twitter.com/ne0liberal/status/1430977537044267008
Being here in CA and la country, no surprise.
La was basically the worst most hard hit sizable metro area in January even with heavy restrictions. We were getting devasted , especially the Hispanic community.
Then by a few months later in May, we were just about the lowest metro area in cases per capita. This wave we have been lower than most places.
Southern CA as a whole basically same pattern.
Texas had had more cases and deaths for the large majority of 2021, but still only just about now making up for big CA lrad from early months.
I would note that choosing january 1 as a starting date is a silly thing that makes the table somewhat meaningless or distorting. Obviously cumulative as Rick is showing is more revealing. But if you want a more recent 2021 start date , something like maybe April 1 or a bit earlier would at least distinguish the delta impact.
What choosing jan 1 does is to bias it to make states whose winter wave started later look worse , which was generally the more Southern states ( where cold weather hit later). And also by eliminating the bad first wave in the spring of 20, make states like NY and NJ look much better than they deserve.
Funny how those biases on average will tend to make more red states look bad . But also a few blue ones like CA.
I want to apologize to you that you, much as El Jefe, had to live to find out that the Rona was not a Blue State Eraser.
"And also by eliminating the bad first wave in the spring of 20, make states like NY and NJ look much better than they deserve."
You mean those states that got slammed when Covid first arrived on our shores, before people knew what was going on, when there were no mask mandates, and certainly no vaccines available, when Trump was president disparaging science on a regular basis, and while he banned flights from China, allowed flights to continue in to NY's airports from Europe (most of the NY strain in that period came from Italy.) You mean that time frame?
All righty.
Yes that period.
Whatever the reason, whether it is a good excuse or not , new york has more deaths than any state per capita except nj.
If you are presenting a table comparing total death rates , new york should be higher than fla.
An excuse about why new york is higher, legitimate or not, is irrelevant to the point I was making.
When I say new york and nj then look better than they " deserve " , I meant deserve simply as to death rates, not "deserve " as in it was their fault.
Actually when I wrote that, I was thinking that someone could take it the way you did but could not think of a different term to use. And then thought it was obvious in context. Clearly was not to you.
But, although I was not addressing this in prior post, how much blame does the NY and NJ govts deserve for policies as to their high death counts, compared to say ca and fla?
Yes, to an extent for the things you mention, ny has some excuse for being high. But you seem to assign no responsibility and that is wrong .
Covid first arrived at our shores earlier not in NY but in wash and ca . One point there is the true original China strain seems to have been less contagious and that is what ca and wash got. The first variant European strain was worse and it appears NY did get that first..so go with that.
" before people knew what was going on" . Sorry bs and do not buy that. Not know as well maybe. But I blame trump, fauci, Cuomo and others for just not taking it seriously enough when they certainly could see a problem coming in time to do more.
When it was only in China, a country much different than ours which was not transparent at what was going on, OK, you could say that likely will not be a pandemic here. We have seen many scares fail to materialize.
But once you could see what was happening in Italy, western transparent nation, how can you assume that we can control it. But still Trumpe, Fauci, Cuomo, etc..were downplaying the threat because we did not yet have many cases. Which was stupid.
Cuomo was telling New Yorkers to go out to dinner, enjoy Chinese new year, when Italy was getting hit and there were some NY cases. No, new york does not get a pass for not knowing. At least as compared to CA. Why did CA impose restrictions both earlier and tougher than NY when it was hit later. If ca could see it coming, so could NY.
And yes, I agree trump should have put travel restrictions on Europe earlier..but if Clinton was in office I doubt she would have either. Not the way politics works unfortunately especially since the swine flu "debacle " ( and Ford did do the right thing and got pilloried for it).
In comparison to fla, NY deserves blame for their insane nursing home policy .
You actually did not mention what I would say is the most fair excuse without blame for high deaths in NYC. The density and the fact that they depend on subway.
Look at the case rates now -- not 16 months ago, now -- in NY vs. your heroic red states of Texas or Florida, or Mississippi or Arkansas, for that matter. It's not even close. Yet New York still has the density and still rides the subways.
Now vs. a year and a half ago.
Your hillbilly friends have no excuse now.
Actually, subway ridership is way below where it was in January 2020. So it is not true that New York "still rides the subways." At the anecdotal level, I now take a taxi to work and our housekeeper usually drives to our apartment.
"Actually, subway ridership is way below where it was in January 2020. So it is not true that New York "still rides the subways." At the anecdotal level, I now take a taxi to work and our housekeeper usually drives to our apartment."
lol
Where did I say it was at the same level at pre-pandemic? Obviously it's went way down. But there's still a lot of people on the NYC subway every day (2.5 million riders last Thursday; 1.1 million on the buses), and it's running 24-hours again.
I'm glad you and your, er, housekeeper have options.
I'm a little shocked and surprised that California has a slightly higher death rate than Texassistan
This chart is for the entire year. Pandemic deaths peaked nationally in January. What the situation has been like the last, say, three months, might in many cases/states be quite different from what was happening earlier in the year.
I suppose January 1 is as reasonable an arbitrary start date as any, but one could just as easily go with Twelfth Night, Groundhog's Day, Valentine's Day, or even the Ides of March if not Independence Day... For those who would prefer tabular form:
State 8/27 - 1/1
Alabama 1485
Alaska 313
American Samoa 0
Arizona 1334
Arkansas 1036
California 994
Colorado 389
Connecticut 663
Delaware 832
District of Columbia 526
Florida 1039
Georgia 1092
Guam 140
Hawaii 207
Idaho 499
Illinois 658
Indiana 729
Iowa 751
Kansas 912
Kentucky 1133
Louisiana 1048
Maine 429
Maryland 666
Massachusetts 841
Michigan 851
Minnesota 445
Mississippi 1164
Missouri 777
Montana 769
Nebraska 334
Nevada 1068
New Hampshire 482
New Jersey 863
New Mexico 955
New York 832
North Carolina 722
North Dakota 362
Northern Mariana Islands 0
Ohio 602
Oklahoma 1345
Oregon 388
Pennsylvania 932
Puerto Rico 347
Rhode Island 774
South Carolina 1001
South Dakota 651
Tennessee 942
Texas 965
Utah 422
Vermont 223
Virgin Islands 280
Virginia 784
Washington 400
West Virginia 945
Wisconsin 547
Wyoming 684
West 833
Midwest 671
South 986
Northeast 824
Pacific 831
Mountain 836
West North Central 647
East North Central 682
West South Central 1017
East South Central 1160
South Atlantic 915
Middle Atlantic 870
New England 697
For those curious about since the beginning and the per-day-per-million 7 day average:
Rank State Cumulative Deaths/million State Cumulative Deaths State 7-Day Trailing Deaths/Million/Day State
1 New Jersey 3020 California 65629 Mississippi 13.82 Florida
2 New York 2784 Texas 56345 Louisiana 13.55 Texas
3 Mississippi 2782 New York 54152 Virgin Islands 11.99 California
4 Louisiana 2659 Florida 43979 Florida 11.49 Michigan
5 Massachusetts 2643 Pennsylvania 28180 Arkansas 10.51 Ohio
6 Rhode Island 2609 New Jersey 26826 Nevada 7.10 Mississippi
7 Arizona 2572 Illinois 26322 South Carolina 6.63 Arizona
8 Alabama 2479 Georgia 22553 Wyoming 6.59 Georgia
9 Connecticut 2344 Michigan 21520 Texas 6.36 Louisiana
10 South Dakota 2333 Ohio 20799 Alabama 6.15 Alabama
11 Arkansas 2265 Arizona 18724 Missouri 5.58 North Carolina
12 Pennsylvania 2201 Massachusetts 18219 Kentucky 5.37 Tennessee
13 Michigan 2155 Indiana 14373 Oklahoma 4.91 Virginia
14 New Mexico 2148 North Carolina 14319 Georgia 4.76 South Carolina
15 Indiana 2135 Tennessee 13338 Alaska 4.63 Washington
16 Georgia 2124 Louisiana 12359 Tennessee 4.25 Nevada
17 North Dakota 2089 Alabama 12153 Montana 3.74 Arkansas
18 Nevada 2089 Virginia 11769 Puerto Rico 3.73 Missouri
19 Illinois 2077 Missouri 10894 West Virginia 3.67 New York
20 Florida 2048 South Carolina 10452 North Carolina 3.54 Pennsylvania
21 South Carolina 2030 Maryland 9971 Delaware 3.52 Indiana
22 Iowa 1987 Wisconsin 8438 Idaho 3.52 Oregon
23 Oklahoma 1974 Connecticut 8358 Oregon 3.49 New Jersey
24 Tennessee 1953 Mississippi 8279 Arizona 3.20 Puerto Rico
25 Texas 1943 Minnesota 7892 Indiana 3.08 Kentucky
26 Delaware 1926 Oklahoma 7812 Washington 2.83 Colorado
27 Kansas 1905 Kentucky 7685 Kansas 2.55 Illinois
28 Ohio 1779 Colorado 7111 Utah 2.27 Kansas
29 Kentucky 1720 Arkansas 6836 New Mexico 2.25 Hawaii
30 West Virginia 1704 Washington 6507 California 2.20 Wisconsin
31 Montana 1668 Nevada 6433 North Dakota 2.06 Idaho
32 California 1661 Iowa 6268 Virginia 2.04 Maryland
33 Maryland 1649 Kansas 5550 Hawaii 2.02 New Mexico
34 Missouri 1644 New Mexico 4505 Illinois 1.94 Utah
35 District of Columbia 1642 Oregon 3115 Iowa 1.90 Massachusetts
36 Wisconsin 1449 West Virginia 3054 New Hampshire 1.89 Minnesota
37 Wyoming 1424 Puerto Rico 2823 Michigan 1.82 New Hampshire
38 Minnesota 1399 Rhode Island 2764 Wisconsin 1.72 West Virginia
39 Virginia 1379 Utah 2623 Rhode Island 1.48 North Dakota
40 North Carolina 1365 Idaho 2327 New Jersey 1.40 Connecticut
41 Idaho 1302 Nebraska 2315 Pennsylvania 1.35 Delaware
42 Colorado 1235 South Dakota 2064 Ohio 1.34 Maine
43 Nebraska 1197 Delaware 1875 New York 1.31 Montana
44 New Hampshire 1041 Montana 1783 Maryland 1.16 Rhode Island
45 Guam 883 North Dakota 1592 Vermont 1.14 South Dakota
46 Washington 855 New Hampshire 1415 Colorado 1.09 Vermont
47 Utah 818 District of Columbia 1159 Minnesota 0.99 District of Columbia
48 Puerto Rico 752 Maine 928 Nebraska 0.96 Alaska
49 Oregon 739 Wyoming 803 Massachusetts 0.93 American Samoa
50 Maine 690 Hawaii 582 Guam 0.87 Guam
51 Alaska 591 Alaska 438 Connecticut 0.84 Iowa
52 Virgin Islands 494 Vermont 275 District of Columbia 0.81 Northern Mariana Islands
53 Vermont 441 Guam 145 South Dakota 0.81 Oklahoma
54 Hawaii 411 Virgin Islands 53 Maine 0.64 Virgin Islands
55 Northern Mariana Islands 36 Northern Mariana Islands 2 American Samoa 0.00 Wyoming
56 American Samoa 0 American Samoa 0 Northern Mariana Islands 0.00 Nebraska
Ignore the state names at the end of each line - a selection/copy error on my part...
If nothing else, you have shown why Kevin's use of graphs is so much better than a pile of text.
Perhaps. Depends on whether one is going for qualitative rather than quantitative. Though as I suggested once before, when Kevin was posting at Mother Jones, he could improve the chart markedly by making it vertical to give/use more screen real estate.
Just think Kevin
Next week sat 9/4 is the start of the SEC college football season
86,000+ fans - sitting elbow to elbow screaming, yelling- Teams like Texas, Arkansas, Mississippi, Alabama, Florida - all with governor's who don't care
All with students from all over the country
They'll have their ICU's empty by then won't they?
Even then, being outside close, won't have the transmission inside being close. It's after the game where the problem lies.
They were advising 6ft clearance for Alpha variant
Delta is 6X more dangerous
I think I'll go to a game and start hawking some approved "product"
"
"Ivermectin - get yer Ivermectin here"
Didn't mr. loser suggest Lysol?
It’s just not the SEC or southern, GOP-led states. It’s pretty much all of college football, including here in PA where over 100,000 will attend Penn State games with no restrictions on entry of any kind. And, the same, I believe for all Big Ten schools,
With the players, coaches mostly vaccinated, nobody cares about the silly fans. Neither would I.
What about your boy Nick Rolovich?
Meanwhile, in pro football, pretty sure January 6th March on Washington attendee Jack del Rio has been discouraging the Washington Football Team roster from vaxxxxing in the hope the immunocompromised head coach Ron Rivera gets a deadly breakthrough case, thus opening the door to elevating Defensive Coordinator del Rio to the head job.
(Of course, del Rio is actually likelier to end up subpoenaed by the House Special Committee on the Jefista Coup than anything else, but no one ever said a MAGA or a USC alum were smart.)
I think you make an important point about the difference between ourselves, Europe and the countries that successfully managed the pandemic such as New Zealand. The successful ones accepted that they are in an emergency and that normal life wasn’t going to be possible for some period of time.
By contrast, every holiday, every sporting event, every Trump rally, and every motorcycle rally in South Dakota was a superspreader. We couldn’t just write off Thanksgiving or Christmas or the annual motorcycle rally for just one year. The predictable spike after every holiday has kept the pandemic going much longer and more seriously than necessary.
It's all good as they're providing free de-wormer next to the beer concession.
I would speculate that this distribution can largely be derived from two factors: red/blue political pattern, and urbanization. You want to be safe, share a state with people who are liberal or geographically scattered, ideally both.
Generally speaking, yes, the bluer the state the safer you will be. But it’s not an iron rule. Without universal public health measures, particularly are regards compulsory vaccination, compulsory masking for unvaccinated people, and the universal requirements of vaccine passports. No community can be safer than its biggest asshole wants it to be.
A case in point:
https://www.washingtonpost.com/health/2021/08/28/delta-variant-unvaccinated-children-elementary-schools/
Just eyeballing the chart it seems that less densely populated states did better, with some obvious outliers like AZ. Maybe this provided a bit of natural social distancing?
Nobody has mentioned yet the new Israeli study which appears to show that natural immunity is dramatically more effective than vaccine immunity in preventing infection, and therefore I assume spread.
I have been saying that for a time here based on what I saw re the rate of spread for different areas. But I was not thinking that large of a difference . Actually I had thought of that and it did seem a good explanation but I just rejected it as I thought that just could not be, but I likely should have not rejected it that quick.
Based on this, and even assuming that the actual truth is not as big a difference as that study shows, it seems more and more likely that;
A) the R0 for delta really is quite high - maybe near 10.
B) the R for vaccinated only ( with current two dose) is still well above 1.0, maybe up near 1.5, which is why it just keeps going on even in heavily vaccinated populations like uk and Israeli.
Even in a 100 % vaccinated population ( with no other immunity) that just will not stop delta.
C) natural immunity will bring R well below 1.0, as we see it doing now some places
D) but immunity does fade- both types- over time. Normal for any virus for antibodies to fade but t cell memory stays. Thus you might eventually get it again but it will be mild.
E) sure looks to me like covid will become endemic. We are simply not getting rid of it or beating it by a vaccine
F) and appears that you need to get covid and thus natural immunity to get a decent long term immunity
G) but the vaccine can get your immune system ready for covid so when you catch it , mild case. Basically when vaccine immunity at full strength, as good or even better at preventing serious illness as long term natural immunity.
H) so, if we all are going to get covid one day, key is I guess to get it the right time and at a low dose.
All this is subject to review as this study is new. And maybe a third booster for mnra will be better so want to see how this works.
But it brings up a few questions which I will ask next post
D)
So two questions I do not know the answer to and cannot find. If anyone who knows immunity understands and can answer, would appreciate.
I think we have all been exposed to the covid virus by now unless you live in a bubble or Antarctica. Everyone has likely inhaled thousands of viruses by now, but maybe not enough to cause a true infection.
If we inhale say a small dose of 500 viruses, and our innate immune system handles it by itself, does that give the adaptive immune system any " head start " re immunity? Any boost that will help it handle an actual infection later?
Or does the virus have to be enough to cause an actual infection to give you any adaptive immunity at all?
Can vaccine immunity prevent you from developing a good natural immunity? I.e. if you get infected and the vaccine type antibodies are good enough to knock it out by themselves, would that mean your adaptive immune system never learns to produce natural antibodies?
Antibodies wane fairly quickly, so I doubt there would be any negative in having antibodies fight off the disease.
As for infection, it's all relative right, what does "infection" even mean? When they do PCR tests, the score is how many times they have to cycle to find relevant RNA traces, so wherever you put the number is somewhat arbitrary, and above that your body could still have been exposed and fought off any further infection. Plus, those traces of RNA just mean the virus was in you, they don't necessarily mean "active" infection (could be traces of infection already fought off).
The best immunity is going to be vaccination and natural immunity from previous infection, and if you haven't already been infected, you definitely want to be vaccinated before infection.
What I was worrying about was if the vaccine antibodies were still effective enough in fighting off an infection, then adaptive immune system has no need to develop the better natural antibodies and you never get natural immunity.
Now, even if that was true , would not mean better to be unvaccinated
It would just decrease the value of vaccination, cannot eliminate it.
And optimal time then to catch covid, if such time exists, would be when it is not effective enough to prevent infection and the immune system has to kick in to develop natural type antibodies . But those vaccine antibodies are still good enough that they slow the infection down enough to give the immune system more time, or the vaccine antibodies, even if not as good, still help in the fight . So you do not get very sick and yet still get strong long lasting natural immunity.
So maybe in the end this vaccine just cannot stop you from getting covid in the end. The immunity is not good enough or long lasting for that. So you are going to need to get covid and develop natural immunity to be protected long term.
But if all the vaccine ends up doing is to make the needed infection for natural immunity fairly painless with a mild illness so you get natural immunity " cheap", well that is still a life saver. I can live with that, if I can figure out how to do that.
See myself I live alone. I could stock up for two weeks and isolate myself after catching covid to avoid infecting anyone else. Nowhere near there yet, but I am wondering if eventually I will want to deliberately catch covid at a time relative to vaccination when the risk of serious illness is minute.
I think you're still missing that the vaccines weren't designed to prevent infection, and the Israeli data is also not being put in the proper context.
Let's take Israel. They currently have a total of roughly 600 people hospitalized for COVID, of which roughly half are fully vaccinated. Sounds bad huh? Except it's not, if you contextualize the actual numbers, and include all the relevant numbers.
And the relevant numbers are that there are 5.4 million fully vaccinated Israelis, with only 300 of them currently in hospitals, a miniscule percentage, and a percentage that lines up with effectiveness claims for the vaccines, which are that they are very high in preventing severe illness and death, which is the metric by which the vaccines were developed and tested.
Also, these rare severe illnesses are even more rarely leading to death, and almost invariably include people over 60. The vaccines are not 100% effective (no vaccine is).
Meanwhile, the other 300 who are unvaccinated come from a much smaller pool of people, which is trending much younger than the vaccinated group in the hospital. So doing the basic math there is no question that you should get vaccinated if not already the case, before taking your chances (risk) on natural immunity.
The troll doesn't understand conditional probabilities. Whadda surprise.
1) On what do you base your contention that "we have all been exposed to the virus" by now? Are you talking the entire world? Certainly in the US it's a very large number, but is it really 100%? Is that just a gut instinct take of yours, or based on any data? Not saying you're wrong, mind you. But I am curious as to your reasoning, If you're right that's bad news, I reckon, because it would imply that very low exposures don't do much good in terms of jump-starting immunity (I mean, clearly in many countries including the US, the disease is still spreading quite rapidly and killing a lot of people).
2)
I certainly don't have the answer to that, BUT, the situation you describe has been posited as a partial explanation for the lower rates of covid reported in many global south countries (in other words it's not solely a matter of under-reporting according to this theory). Basically, people living without air conditioning in tropical climates keep their windows open/and or spend much time out of doors. So (goes the theory) such people are likely to get "micro-dosed" with coronavirus virions — not enough to give them the disease (and maybe not enough to give them a detectable infection?) but enough to stimulate their immune systems.
Just to elaborate on my question regarding 100% population exposure: I believe it's increasingly clear by now that this is where our species is headed. I just don't have a good sense as to when arrive there. You seem to think it's already happened. I'm just wondering if it might by, say, the summer of 2022, or the autumn of 2023 (or whenever).
First, just to clarify, I am using the term " virus" in the way it is commonly used. Some scientists feel " virus " is really the infected cell and the things that go out to infect us should be called a "virion ". You can look that up if you want an illustrative explanation.
So the estimate of number of viruses or virions in a human who is infected is 1 to 100 BILLION. And they are exhaling them into the air all the time. Over the last year, with at times maybe up to 2 or 3% of the population being infectious at the same time, exhaling millions of viruses into the air, you do not think you have breathed in a few. These things are incredibly small and very numerous. Do you know all of the covid virus in the entire world would fit into a can you could carry around with you?
Even if you are in an enclosed room with all windows shut, air seeps in ( otherwise you would eventually die from lack of oxygen) . Only specially sealed rooms like those in labs are sealed off well enough to really stop viruses.
So unless you have not been within a mile of another human being for the last year, you certainly have been exposed to the virus. Have probably breathed in many thousands of them.
But that is what the innate immune system is supposed to take care of - it knocks out random viruses and bacteria all the time, every day, before it can really " infect" you and it can get around it and start multiplying. If it does, then that is a job for the adaptive immune system .
At least this is my best understanding.
And maybe different levels. A mini exposure where the innate immune system kills the virus before it can infect a cell probably happens all the time I think. But I expect that would do nothing to start the adaptive immune system and get any natural immunity.
Note we all have " innate immunity " from the innate immune system built in. But it does not adapt and learn like the adaptive immune system . So what is commonly referred to as immunity is really adaptive immunity. Innate immunity is a given.
What you refer to as micro doses are, I believe, a small dose of the virus but one which does get past the innate immune system and a very small number of cells are infected. But so small that the adaptive immune system kills it off easy enough. I expect that, for most of those, this has happened too.
But will this little micro dose trigger the adaptive immune system enough to learn anything? I expect the body will not keep making antibodies so serology test will show nothing . But maybe enough memory so more prepared to start making them?
Wow! These are a lot of daring conjectures from one single study--from Israel whose results seem to differ consistently from anybody else's.
One point I am sure you are getting wrong: We have by now had about 39 million documented cases in the US (via Google). Let's say twice as many cases were missed due to insufficient testing and asymptomatic cases. That would get us to approx. 120 million infections. This is still only about a third of the population. I believe we have to assume that the majority of vaccinated people have not had a natural infection as well.
Another point I want to make: Delta is different from the strain that the vaccines were designed for. So what we are observing, or better what all these studies are observing is a mixture of two effects: The natural waning of immunity over time and the reduced immunity of the vaccine against delta (which is now the dominant variant and will probably stay dominant for quite some time*). In the media at least those two effects are constantly mixed up and one never quite knows which of the two effects is being talked about. But for a clear analysis one needs to keep the distinction in mind.
I would very much prefer to have a vaccine that is redesigned for delta rather than a booster of the same old vaccine. Such a vaccine would likely get R0 below 1. But everybody seems focussed on the booster. RNA technology is supposed to make such a redesign easy and much quicker than the chicken egg technology they are using for the flu shots (where they manage a new design every year nonetheless).
* Delta is a much "better" virus than the other variants; it will be harder for any new variant to beat delta than to beat the other variants. So delta it likely is for some time to come. Which means designing a vaccine against delta is a good idea and should be high priority.
I agree with most of your points some strongly. But others not as much.
First , daring conjectures from one study . Not really.
What were daring conjectures were what I had before where I was trying to infer what vaccine and natural immunity might be from comparing Rs of different places vs their levels of vaccination and presumed natural immunity. That was " daring" but it was all I had to go with . There were no studies anything like this Israeli one ( and why the hell not - why is little Israel the fitst nation to rigorously study this?).
When I was doing that, I was saying that it really did look like natural immunity had to be better than vaccine. You just could not explain why the high vaccine places did not have a much lower R otherwise. But I sort of censored my guesses. It did seem that data fit best with natural immunity being far better. But I was just reluctant to think that ( after all most here were telling me that vaccine immunity was better).
But I was never thinking of anything like 13 times better. I think at one point I got 5 times better but then tweaked my other assumptions to get something more " reasonable". Looks like a tweaked the wrong direction.
Re number of infections. Why are you saying you are " sure " I am wrong. That is arrogantly ridiculous to say you can be sure of the number of total cases . Nobody knows. Actually from your overall tone I think you were just being hyperbolic there and not as arrogant, I hope. No way you can be sure that there are only 2 missed cases for every confirmed. If you just presume something by " saying "it is so , you can be sure of anything . One problem with serology tests is antibodies do wane and sometimes to undetectable levels but we are not testing for t cell immunity. So serology will underestimate number who had covid . But we do know from early that number of undetected cases was way higher- like a multiple of 20. Now lower maybe less than one missing for each confirmed. Who knows re cumulative.
But even more you cannot say you are sure I am wrong because I never said the infected %age was over 1/3 in latest posts. I still do think it is higher . Latest study ( although it uses modeling not hard statistics as no measurement of tcell) indicates total infected in usa of over 50%. Are you saying you are sure those scientists are wrong too?
But the thing is the Israeli study does imply a lower % age of total infections ( i.e. lower % with natural immunity).
We know vaccination rate in US places . We know pretty well the R . We need to know three other things to make the math fit ( i.e. to get that R observed result). The R for natural immunity, the R for no immunity and number with natural immunity ( actually also need immunity overlap and double immunity R but ignore that for now).
So to get the R , knowing vaccine R, the other three factors have to " add up". Well now we have a number for natural immunity R implied and it is much lower than I earlier thought, almost so low to be effectively zero.
And what that means to get the R is that either you have to adjust the no immunity R up or the natural immunity % age down.
But we do have real data on comparing no immunity R ( at least infection rate part ) vs vaccine R . So have some solid guess there.
The piece where we have the least hard data is the %age infected. So makes most sense to try to infer that one.
When I tweaked the assumptions earlier to get the numbers matching the Rs , in order to get the natural advantage down, I was tweaking the estimated %age infected up . But there was having trouble as needed way too high numbers like almost 100% some places . I just have just stuck to my initial and realized that yes natural immunity is great.
I agree with your 3rd paragraph. But would say that it looks like the reduced immunity for vaccine for delta is just an issue of it overall reproducing faster - i.e same thing allowing it to be more contagious vs unvaccinated. I see nothing indicating that delta is avoiding the vaccine immunity itself- it just works better overall.
So designing a better vaccine against delta just means designing a better vaccine overall- one that works better against any strain.
And not sure how easy that is. I think might require a whole new approach like not targeting the spike and trying to mimic natural antibodies targeting the whole virus? I do not think that is just tweaking the existing virus.
I do think you seem to be on my page re the threat of variants. Delta is an extraordinary good mutation. Makes it hard for a future mutation to beat it. Many seem to think a variant like delta being such a huge improvement means you should expect future jumps as dramatic while it would indicate the opposite.
Actually if we saw another hugely more contagious virus , we have to start worrying about whether variants are being manufactured by China or someone else.
Re vaccine resistant variants, where the variant specifically avoids the immunity, not sure how good the mnra vaccines are.
On one hand, I understand the point of targeting the spike is that it is an essential thing the virus cannot do without. Cannot simply evolve to eliminate the spike as it needs it to infect at all. Any non spike mutation would not infect anyway. So to that extent the vaccine would be " variant proof".
On the other hand, having the antibodies focused on only one thing gives any mutation one thing to beat. Like maybe keeping the spike but hiding it so antibody does not recognize.
Natural immunity is always going to be harder for a variant to really avoid. As it recognizes all parts of the virus, and the virus cannot mutate everything, a variant can weaken immunity a bit, but not avoid it that much.
I had thought they were saying natural immunity is greater in regard delta as opposed to vaccine immunity, but didn't characterize vaccine immunity as being worse against other variants.
Well I was coming to that conclusion looking at the rate of infections ( i.e. how fast cases were increasing) at a time when delta was dominant so my earlier conclusions based on that would have been with respect to delta.
I was not trying to do such analysis before delta. Not sure if our differentials in vaccine rates were high enough to try to imply that way before delta.
I think the Israeli study was largely before delta ( they had vaccinated more there before delta hit) but not sure. But see little reason why we would expect different results.
I would expect any immunity to be worse against delta as it seems Delta's advantage is mainly just in producing higher viral loads and not anything specifically getting around immunity itself. So I would expect that delta would change both about the same proportionately.
As to my personal concerns as to whether this Israeli study will hold up, especially as to the extent of the greater effectiveness ( like SIX times more effective), I wonder about a few things. But just do not have the expertise to review this myself and waiting to see any responses from scientists bringing up these issues.
One is that, because the study compares three groups, one being those fully vaccinated, one with natural immunity, and one with single dose and natural immunity- but not double dose and natural, i have to guess they just did not have enough data of anyone with full vaccine immunity and natural immunity. So I would think that maybe this was an early study .
But then occurs to me that maybe natural immunity kicks in quicker- i.e. it is at a peak right after you recover. But maybe vaccine immunity takes longer to build up to full strength before fading.
So maybe they were looking at a time frame that was somewhat unfavorable for the vaccine?
Note they did take into account how long natural immunity was from. The advantage of natural immunity over vaccine was less ( as you would expect) looking at all those with natural immunity ( including those who got it nearly a year prior) vs. Those who had covid more recently.
I always want to try to assess the arguments best I can so want to see anything from actual scientists that gives reasons to be sceptical. So far have not really found anything. If anyone knows of any such, I would like to hear.
Keep in mind this is only one study, I don't even know if peer-reviewed yet, it's not necessarily universally applicable (UK seems to have different data), and there's not a lot of precision in really knowing the complete set of people who have already been infected (as opposed to people who actually got disease, who are more easily accounted for, yet still not precise, and could be that disease-level results in deeper natural immunity).
Let me give a shorter response. When I looked at it, I think it was the opposite.
I believe the data came from the period in Isreal before delta hit Israel and so is showing natural immunity was far more effective before delta at least.
No, cld, read up more and you were right.
The study was for a period when delta was dominant so it is showing that natural immunity was far more effective than vaccine against delta.
But I have to wonder why, it appears, they compared those with only natural immunity, those with only vaccine immunity, and those with natural immunity and one vaccine dose. But not those with full vaccine ( two dose) and also natural immunity. Or maybe they did and the summaries I am seeing do not include it?
Some do say that this might mean that if have natural immunity, one vaccine dose is enough. They did find that one vaccine dose did improve natural immunity. So maybe the two does plus natural group did no better than one dose plus natural?
Given that
If you want to look at the study rather than summaries of it, it's here: https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.full.pdf
"Nobody has mentioned yet the new Israeli study which appears to show that natural immunity is dramatically more effective than vaccine immunity in preventing infection, and therefore I assume spread."
Perhaps because the adults have better things to do?
rolling eyes
Wow.
Such an adult attitude.
Yes, glad you noticed.
Do you really want to pretend that a superficial study pushed by the radical right this week has any significance?
Stay safe
Do you just assume that anything that might not fit what you thought before has to be "superficial " or do you have a reason for thinking so?
I did say, if someone knows of anything giving actual reasons to dispute these results, please cite them. I hate to just assume something is correct before I can hear what someone who disagrees says.
Basically I try to keep an open mind. There have been way too many studies , including ones " pushed " by left or right, that have turned out to be flawed.
If you have an actual reason for thinking this study is wrong, please try to be adult enough to explain or give a cite or something. I want to know , really.
And this did not come out of some conservative think tank. Are you even actually aware of the study we are talking about?
The study is flawed and pretty useless.
@projectbuchanan needs something to do, now that Twitter has cancelled the America First feed over alleged malicious attacks on trans people.
That's a preprint. I hope you read it before commenting on it. -- https://bityl.co/8RSW
I just can't see how people who were vaccinated had a 13x higher risk of infection compared to people who'd previously had an infection; it just is too absurd.
CDC: "Kentucky residents with previous infections who were unvaccinated had 2.34 times the odds of reinfection (OR = 2.34; 95% CI = 1.58–3.47) compared with those who were fully vaccinated" -- https://bityl.co/8RSK
Oh, I forgot to mention that there are lots of other weirdness going on in their paper. I'm not going to say anything because most of the people who leave comments on KD's blog think they're smarter, so I'm sure they'll be able to point out all of the errors so that I can learn from them.
Your comment that you are waiting to learn only makes sense if you think those others really are smarter than you, not just that they think they are smarter.
If you see things that are weird, please explain . And not just wow I cannot believe 13 times . That floored me too at first. But why is it that hard to believe?
We are already seeing that vaccine immunity just is not as effective against infection as we hoped it would be . It certainly cannot be seeing what we are in Isreal and the uk. So saying that natural immunity is 13 times better than vaccine immunity is really what you should expect . Note the 13 times was for more recent natural infection - it was 6 times for the older ones ( so clearly it does wane).
Consider of the R0 is say 8 and vaccine immunity is 50% effective ( 2 times factor ) for both infection and infectious when infected ( so reduces spread by 4), then the R vaccine is still 2.0 and it will just spread and spread.
So if natural immunity is 13 times better, maybe the R for recently infected is .15 or so. Of course. When has a virus ever ever not stopped dead in its tracks if everyone had a recent infection. Otherwise would be unprecedented.
In their first model:
257 infections
238 from vaccinated group
19 from previously infected
256 number difference of immunocompromised people between vaccinated group and previously infected
Point is, the difference in the number of immunocompromised people could explain the gap between infections of the vaccinated and the control group.
They could have easily controlled for the state of immune system, but chose not to. That seems weird if you're trying to ascertain infection risk, don't you think?
I guess I need to explain that last one.
We know from several studies that the mRNA vaccines induce Spike antibodies and neutralizing antibodies at least at the level of natural infection, but generally, elicit higher levels of antibodies.
We also know from recent research that higher antibody levels correlate to better response and protection from COVID-19 infection.
THAT is why one should be highly interested in controlling for the state of one's immune system. We know that immunocompromised people have low levels of antibodies elicited by vaccines. That is why boosters are now recommended for immunocompromised folks.
They cherry picked cases and then put a %%%% on them. It's a bad study. Why it was made, should be the big question. I have my suspicions.
Are you referring to the Israeli study or the Kentucky cdc study?
Either way, on what are you basing the cherry picked comment.
I see no such indication In either.
Re the Israeli study , the exact opposite.
Note they first identified the groups and divided them by status. BEFORE they determined how many got infected during a later follow up period.
You cannot cherry pick a group that way unless you are psychic or have a time machine.
Unless you are saying that you just think they made up the data . Maybe because they are jews or something.
You are misreading that 2nd paper you cite. No surprise and not blaming you there because it has been misreported widely in the media and the cdc itself seems to have been describing it in a misleading way ( deliberately?).
But just read what it says. They compared vaccinated and unvaccinated in a group that had already been infected. What that cdc study was showing is that the vaccine reduces infection by adding to natural immunity. It was not comparing those with only natural immunity but vaccinated immunity with those that only have natural.
So not relevant to whether natural or vaccine immunity is better.
I do see two things now that address both of the things that gave me some scepticim.
One was whether they gave the vaccine enough time to be effective and the other was why they did not give info for a group that had natural immunity plus two vaccine shots.
But the groups were initially chosen months earlier and, at that time, Israeli policy was to only give one vaccine shot to someone who had been previously infected. So that explains why they did not include that group. They had none. But, if the cdc study is correct, we can infer the result because they did compare natural immunity only to natural immunity plus two vaccine shots.
And they did then wait months before the period when they dertmined number of reinfections. So yes they have vaccine time to be at peak effectiveness.
Two remaining quibbles, mostly semantic..
They concluded that natural immunity is both better and more long lasting than vaccine immunity. But they did not measure any group which would compare different vaccine times to see if vaccine immunity wanes.
What I think they meant was that natural immunity was better and that advantage was long lasting ( i.e. natural immunity a year old was still better by far than vaccine immunity at its peak). That is not the same thing as saying the natural immunity is more long lasting. Maybe it is but do not know from this.
Second they did mention one issue which was that they could have missed asymptomatic cases. One thing that makes me more comfortable with studies is when they mention possible problem issues themselves. But it seems they were talking about missing asymptomatic cases in the measurement of infections period. Yes that could bias the results to the extent that one type of immunity had a greater proportion of missed asymptomatic cases ( if the proportion was the same, no bias due to missing cases) . And, since they also found that natural immunity has an advantage over vaccine in preparing serious illness of those infected, it would maybe make sense that it would also have an advantage in preventing minor illness in someone infected. So that could bias the natural advantage on the high side re infection but the low side re serious illness.
But did not address missing asymptomatic cases in initially establishing the groups. That could bias but in opposite directions. First some of the " only vaccine immunity" group could really be " both natural and full immunity ". Obviously nobody in natural only group had missed double immunity. That understates natural advantage. But the " natural only " group is really " natural by confirmed case". To the extent natural immunity is better In those who recover from a symptomatic illness, that biases the other way..
Plus the vaccines were not primarily developed and tested to prevent infection, so it's weird to predicate some study on them versus natural immunity preventing infection.
The vaccines are designed to prevent serious disease and death. This is what studies should be primarily focusing on if comparing vaccine and natural immunity performance.
To my knowledge, there's only one vaccine out of all known vaccines that prevent infection (PPV I think).
Although it was the case that these spike protein vaccines were remarkably good at preventing infection too, at least while the antibodies were still strong, and I guess this spoiled us some in how we assessed the vaccines.
I think you're giving vaccine developers credit for more precision than they are capable of, and consequently blame for the imperfections. They developed vaccines to combat the virus as well as possible. The ideal would have been to entirely prevent covid infections for life; however, results that fell short of that ideal still give significant protective effect and are very much worth having.
In short, I do not believe the developers deliberately limited the effect of the vaccines. They did not design them just to prevent death and serious illness. They designed the most potent, effective vaccine they could develop.
I agree in part, you try to make best vaccine you can, but the success of clinical trials was reduction of serious illness, so ultimately that will be your driver, whether charitably minded or for-profit. There was a limited window of time, and they had to show effectiveness, and for clinical trials this was preventing serious disease.
As of Friday, the Province of British Columbia, reports nearly 700 new cases a day, mostly delta. 75% of the eligible population is fully vaccinated (majority Pfizer, minority Moderna, small number of Oxford/AstraZeneca) and 1% of new cases are occurring in fully vaccinated people. In other words, the case rate among the unvaccinated is 300 times as high as among the vaccinated.
It looks like the vaccines reduce the risk of symptomatic covid, against the delta variant, by 99.7%.
Oh, you mean, "British" Columbia, of Neoliberal wimp Justin Trudeau's "Canada", which is a western province fully compromised by incursion from the People's Republic of China that intentionally leaked a bioweaponized respiratory infection from their Fauci-funded lab in Wuhan?
Yes, I trust their numbers.
Except that I've noticed over the past year that there have been two battling Israeli research groups (one group I call the pessimists about vaccines and the other group I call the optimists about vaccines). This was a study released by the pessimists, and optimists are questioning the pessimists' conclusions. Waiting to see their response to this study.
Oops. I seemed to have replied to the wrong comment.
Hey, conservatives!
You know what kills covid?
Cement!
It crushes covid! Smashes it dead!
It's a simple and straightforward solution, a solution they don't want you to know about!
Your body, your choice.
And it's available to everyone. All you do is buy cement, just like you can find in any store in America. You put a reasonable amount of it in a glass of water, or a glass of juice, or even milk, like you're mixing up Ovaltine or something, and then you drink it! It's as easy as that.
Once a day, a big glass full, for a week. Take it whenever it is you happen to feel like you think you might be coming down with something.
As a Duck Dad, I tend to notice Oregon stories… https://www.oregonlive.com/coronavirus/2021/08/tillamook-josephine-counties-request-trucks-to-hold-bodies-as-covid-19-death-toll-climbs.html
Sympathies on being a Duck Dad. I am a Duck Uncle.
Go Huskies!
Should have gone to Reed.
I heard psilocybin mushrooms & ecstasy offer alternative protection against the Rona at least as strong as Fauci's Faulty Shot.
Pffft!
What the....are half of us from Oregon?
Another duck here. 🙂
I grew up in Oregon and never heard of a Duck Dad. What is it? And are there Duck Moms?
Bear in mind I left the state in '77. Or was it '78?
There are indeed Duck Mom’s. We have one of the small buttons to prove it 🙂 As it happens, the Duck Mom in the family has been to more Duck games than this Duck Dad. Of course the main draw was to see our Duck Daughter (?) performing in the color guard at halftime 🙂
I am picturing this quite literally.
We look nothing at all like Howard.
Anyone here?
https://2.bp.blogspot.com/-HoS4v4VAjJs/USSKuqmYG0I/AAAAAAAAPBY/3x0lwo0I84k/s1600/775654_528791233807563_670338823_o.jpg
Jimm,
Where is this meme that the vaccines were not intended ot expected to prevent infection coming from? They sure as hell were presented that way .
If they are not preventing infection, then they are not going to be effective in stopping you from infecting someone else. In fact, they could actually be HARMFUL in that regard ( I e. Effect on overall community) . If the vaccine does not prevent infection but is good at preventing illness, vaccine works good for the taker but can harm the community . Because then you could be MORE likely to spread the disease to someone else because you will be less likely to know you are contagious and will feel OK enough to be out in public.
Either all the condemning of the unvaccinated for being selfish and harming the community was a load of crap, because you had no reason to think they were hurting anyone but themselves.
Or this " we never expected the vaccine to stop infection " is a load of crap now . And it is the latter.
And why spin this way? New data come in and we revise what we think. Yes, it is disappointing that the vaccine is not as good as we thought re stopping infection, but it still does to a lesser extent. And it works even better than we initially thought re stopping serious illness . So we just need to adjust to that new reality.
It is like the vaccine is now a political candidate and some think they are in charge of doing the spin for them.
And I think you might be confusing the fact that few vaccines produce sterilizing immunity which stops infection ( although I think there are more than pcv) with the idea that few reduce the chance of infection. Many vaccines do reduce the chance of infection and spreading, they just do not shut it down entirely. No we did not expect the covid vaccine to stop all infections but we did think it would be doing better than it is.
The effectiveness of the vaccines against infection or transmission has been a known unknown, as reported as far back as February by the New York Times. The most important thing to most people back then was that the vaccine could greatly reduce their chance of becoming seriously ill with covid-19. The open question about whether the virus could still be passed along by vaccinated got less attention, but it's not a concern that has just come out of the blue now.
https://www.nytimes.com/2021/02/23/opinion/covid-vaccines-transmission.html
[A]ccording to the clinical trial data, both the Pfizer-BioNTech and Moderna vaccines are highly effective at preventing Covid-19, the disease, but it’s unknown how well they prevent infection with SARS-CoV-2, the virus.
Honestly, we're heading a lot of bad science, and bad science communication. Vaccines are not generally designed and developed to prevent infections, they are primarily designed and developed to prevent severe disease and death, with the next level down being symptomatic infection (disease), and in very rare cases even providing sterilizing immunity (against infection).
Very few vaccines in the world provide sterilizing immunity, and sterilizing immunity was never an expectation or promise of this first round of COVID vaccine development.
https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/covid-19-vaccine-what-you-need-to-know?amp=true
https://theconversation.com/coronavirus-few-vaccines-prevent-infection-heres-why-thats-not-a-problem-152204
https://www.scientificamerican.com/article/vaccines-need-not-completely-stop-covid-transmission-to-curb-the-pandemic1/
Smallpox vaccines do not provide mass immunity from the disease? As for the mRNA vaccines, they have been reported as reducing the chance of infection by 95% (pre-delta) as well as reducing severity if infection does occur. What the intention in designing was seems to be irrelevant with that kind of result.
The critical thing would seem to be stopping pandemics and elimination of the disease. Why get hung up on semantics, or what the design intention was?
Smallpox vaccines didn't provide total immunity. It was giving a mild case of the disease to stop bad cases. Boy, I bet the 100 million plus meso-Americans, wish they knew about that.
Also note I'm not saying vaccines can't or don't reduce infection and/or transmission, just that the primary aim is preventing severe illness and death, and the standard for testing the COVID vaccines for approval was primarily this.
And on that note, the vaccines are still highly effective, including in Israel, due to memory t-cell immunity which often with many vaccines lasts for years.
https://www.news-medical.net/amp/news/20210719/Do-mRNA-based-COVID-19-vaccines-induce-memory-T-cell-response-similar-to-natural-infection.aspx
https://pubmed.ncbi.nlm.nih.gov/12531640/
https://www.nature.com/articles/s41467-021-22036-z
I don't think you were paying proper attention to what the FDA (and CDC) said when they approved those vaccines. The vaccines were never billed as 100 percent "preventing infections." It seems to be only the die-hard anti-vaxxers who claim the vaccines were supposed to be 100 percent effective (and that anything less was a failure).
When the Pfizer vaccine was approved back in fall of 2020, it was stated that the Phase 3 trials indicated a ~95% effectiveness against the SARS-CoV-2 variants in circulation at the time of the trials. 95% effectiveness meant that for 95 out of 100 vaccinated people it could prevent a breakthrough infection (and breakthrough meant an *infection with symptoms* by the definition of effectiveness set by FDA). The J&J P3 trials indicated that it would be slightly less effective (~86%, if I recall correctly). And the data for all three vaccines indicated that the vast majority of breakthrough infections would *not* result in hospitalization or death.
Now, with the Delta (B.1.617.2, Indian) variant, we're seeing real-world epidemiological data (not in vitro data) that all the vaccines combined are running about >80 percent effective. Which is still pretty damn good.
Also, as soon as the Alpha (B.1.1.7, British) variant started to spread (end of 2020, beginning of 2021), experts were saying we'd probably need a booster. So boosters have have been discussed since at least Dec 2020. Just so you're clear on that point. 😉
I think I do not want to keep belaboring this issue with Jimm as it seems the differences ( where he is wrong) are largely re semantics or where it really does not matter much now ( who cares now what was intended when we see reality).
But qx49 summarizes the history accurately I think. Phizer sure as hell promised us real good effectiveness at preventing infection in the person taking the vaccine.
And the not as good results are not just because of delta. I think phizer played a few games that oh just coincidentally made the vaccine they developed look better. What a shock, right? Now not saying they faked the data but drug company studies will tend to show results and use criteria in their favor. And then describe them in ways that are not lying but might mislead an average person to assume it is actually more than the results.
You can read online plenty of criticisms in that regard but I will expand on one thing qx49 mentioned.
The study reported 95% effectiveness in reducing symptomatic infections but did not look at all infections including asymptomatic. Since we had concerns re asymptomatic infection from the start, is it not odd that they did not even try to see how effective it might be with asymptomatic infections that could still infect others? They could have had a smaller subsample that they randomly tested to detect those. But did not. Why?
You think maybe by reporting 95% effectiveness at stopping symptomatic infection, phizer might have realized that many would take that as reducing all infections by 95% and thus reducing spread by that much ( which is what happened)?
I never bought that inflated 95% figure from phizer re original covid either.
In a way phizer lucked out with delta. Gives an easy thing to blame. If we were seeing real world data on original and no variant happened, I think we also would be seeing less than phizer study and they wollf have some explaining to do.
> If they are not preventing infection, then they are not going to be effective in stopping you from infecting someone else. In fact, they could actually be HARMFUL in that regard.
Wrong. A bunch of studies have shown that the level of virus shedding is lower in people with breakthrough infections than people with unvaccinated infections. Thus a person with a breakthrough infection is much less likely infect someone (effectively reducing the R value of virus in vaccinated people).
Also there are pre-COVID studies for measles that show that vaccinated populations tend to protect the unvaccinated.
Ha,
OK you got me pn semantics but not really are the actual issue.
This sort of thing is why I posted at 11: 14 am today ( before your above post) to clarify my terms.
With the terminology I am going with now re that post, and the post I made you are criticizing, your point is 100% valid. If you read that post , you will see I make the exact same point.
Using the terminology from my 11:14 post today, my earlier post should have read that if they are not effective in preventing spread ( my category #3 including reducing infectiousness), then they do not protect you from infecting others ( duh redundant).
My point was Jimm was saying they were only intended to prevent the vaccine taker from getting sick. But that alone does not prevent the spread or contribute to herd immunity.
So if it was not expected to reduce spread, by reducing infection, reducing infectioysness , or combination, then all the talk about using the vaccine for the good of the community and for herd immunity was bs that fauci was pushing . But it wasn't. They expected and counted it to work that way.
And it still does, just maybe not as well as we hoped. I think we agree there.
As you say studies show the vaccine does reduce infectiousness. Yes, some studies seem to show that at the peak a vaccinated breakthrough infection might have the same top viral load ( and I am still suspicious of the methodology) but also clear that it declines faster. So just maybe a breakthrough infection is as contagious at its peak but still less contagious for the life of the infection.
Agreed?
D ohrhk,
Does not seem I can reply below you so posting at bottom.
You did not need to explain further. I had got your point.
But think you are wrong.
They did control for comorbities. They ran a multivariate regression. And they said right in the paper that the multiple was adjusted for the other factors ( which also included things like age and sex and SES). And since the two groups were the same size, you can calculate the unadjusted ratio of 12.52 or 238/19. Not their final 13.06.
And they also mentioned that they did not see that comorbidities were statistically significant except for 60+.
And no way could you possibly expect the immunocompromised difference to explain it all even if you only had the numbers. Just try to work through the math. The TOTAL number of infections in the natural only was a frigging 19... just 19!. There is no possible way to distribute the numbers based on immunocompromised that could account for 238 vs. 19.
Try. Make up whatever distribution you want . Cannot be done mathematically.
No. They controlled for only the things that are 100% matching in their profiles between the two groups of each model.
I think you are wrong. Will post later on this and other things with you.
This summarizes some of the questions/debate surrounding the natural immunity vs. vaccination immunity debate, and touches upon the booster shots issue, as well as the desirability/need (if any) to vaccinate children:
https://www.bbc.com/news/health-58270098
That is a pretty good article. Explains some things in an understandable way .
I would note that it came out before the Israeli study and so does not take that into account. So it does not actually say anything about concluding that natural immunity is better or not as compared to vaccine. But it does give an explanation as to why that could or should be so.
It sounds like someone who was thinking and expecting that natural immunity really was better and getting frustrated at the incessant statements that they had proved that vaccine immunity was better ( which were always crap).
One thing I noticed was the early statement that all discussion of the possibility of natural immunity being better ( in fact any discussion of natural immunity at all often) was seemingly being suppressed by much of the media and scientific establishment. Which was really bad.
I doubt the Israeli study was much of a surprise to serious epidemiologists looking at things in an unbiased way.
And his statement at the end about the vaccine maybe being really useful as a way of minimizing the impact of an actual infection - which you might need to get the better natural immunity. That is really what I am getting at . And think maybe that is where we are going.
Look at it this way. Early vaccines were often taking actual live viruses and infecting you ( i.e. they caused an infection) but weakened ones so the sickness was mild and it was not very infectious.
So maybe all the covid vaccine will do is effectively weaken any actual virus in a subsequent real infection, basically same result..and we can live with that even if it means we still have to catch a mild case of covid.
1) Survivor bias. Literally. The prior-infection group in the Israeli study included only those who tested positive _and_ _ lived_. You can’t match S’s across groups on factor ‘would not have died’.
2) Even if we took this study as definitive (and no single study in any life science is ever definitive, IMHO), what would we do differently? Not be vaccinated, wait to acquire Covid-19, because natural immunity is ‘spectacularly better’? When multiple studies have shown that p(death | vaccinated << p(death | not vaccinated)?
*sorry, iPad doesn’t do a proper vertical bar to represent ‘given that’)
Like some others, I don't understand starting the dataset at January 1 -- when virtually no one had been vaccinated. The chart would be far more informative if begun before the start of the current wave while immunizations were already widely available to nearly everyone. Just eyeballing the Worldometer 7-day average for Covid-related deaths, the low point looks to be around July 8 before it started going up again. That way we could better evaluate the effectiveness of each state's and its residents current mitigation efforts.
I am vaccinated, take care to avoid risks and, so far, I haven’t gotten the plague. This dude was not vaccinated and protested mask recommendations. He’s dead now. Good riddance.
https://sanangelolive.com/news/health/2021-08-28/freedom-defender-caleb-wallace-dies-covid-19
SAN ANGELO, TX — Caleb Wallace, the San Angelo man whose life came to define the revolt against government overreach in Covid-19 restrictions, died today of Covid-19. He had been at Shannon Medical Center since July 30.
Maybe some day I’ll get a breakthrough infection and suffer or die. Who can say? While everyone debates these trivial details, I’ll just hunker down and stay out of the way. Good luck.
Ah, this age, so modern and yet so primitive! Kudos to Rick and company on the limitations of this representation. Dashboards and Pandas are mainly what I teach to in my data science bootcamp these days (my students typically don't have the statistical chops to do any but the most minimal analysis), and what would be nice would be to have something a bit more interactive; a chronological slider, say, starting 2020.01.01 and ending with the most currently available data.[1] The bars are fine for what is being portrayed, but I'd use multiple bars, one for deaths per million, another for percentage vaccinated.
Here's a link to some chart suggestions for the type of information you're trying to convey.[2]
[1] We teach interactive JavaScript for this one. JavaScript is ... not to everyone's taste, and I can see why Kevin doesn't use it.
[2] Yeah, Matlab. Sue me, I'm old. But I don't use it much any more either.
Another one down…
A conservative radio host from Florida who criticised coronavirus vaccination efforts – and called himself “Mr Anti-Vax” – before contracting Covid-19 himself has died, his station said on Saturday.
A statement said: “It’s with great sadness that WNDB and Southern Stone Communications announce the passing of Marc Bernier, who informed and entertained listeners on WNDB for over 30 years. We kindly ask that privacy is given to Marc’s family during this time of grief.”
When Bernier was hospitalised with Covid-19, three weeks ago, WNDB operations manager Mark McKinney told local media: “If you’ve listened to his show, you’ve heard him talk about how anti-vaccine he is on the air.”
When our mortal enemies are themselves killed, it makes us safer. Keep it coming.
I doubt he is really anti-vaccine. More or less a dialectical warrior. If mainstream liberals had been against the vaccine, he would have been for it.
Well… He is dead now. If it speaks just shtick, then he pulled it off to perfection. So I think he WAS anti-vax but now he’s just dead. Ding dong..
If it was just shtick…
Nope, it is a con. Everything is a con with you bourgeois humpers. Why the reactionaries of capitalism think this "anti-vax" stuff means anything is head scratching. It doesn't play politically and as a pandemic spreads and evolves, continues to undermine the con.
Give it up and tell your elites to go back to pre-2010. Bad move to mimic the old left.
And he’s still dead. Some con.
Many factors affected infection and death rates through the middle of 2021. If you want to see the effects of different state vaccination/masking policies, start the count around July 2021, when large numbers had been vaccination in some states, and when the delta variant became important.
I am puzzled. This data does not match what is being calculated for Missouri (and nearby states). Please check out the chart titled 'Reported COVID-19 Mortality By State' at https://slu-opengis.github.io/covid_daily_viz/states.html .
First , in response to various and especially Jimm, let me clarify and explain something .
I will define the vaccine as being effective in four ways.
First in preventing infections - i.e. reducing infections in those who took the vaccine.
Second in preventing infectiousness. - i.e reducing the chance that someone infected will infect someone else.
Third, in preventing illness - i.e. reducing the chance that someone infected will become ill ( with various levels from minor illness to serious to hospitalization to death).
Fourth, in preventing the spread of the virus - i.e. reducing the R and how fast cases in increase or decline. This is a factor of two of the above things - the effectiveness in preventing infection and the effectiveness in preventing infectiousness. If the vaccine cuts the chance if infection by 50% and also cuts the chance of infecting someone else if you are infected by 50%, then it will reduce spread by 75%. .5 *.5 = .25.
Fifth, in preventing amount of illness- I e. Reducing total number ill. This is a combination of the above categories of preventing infection and preventing illness. If the vaccine is 50% effective in preventing infection and 90% effective in preventing illness if infected, it will be 95% effective in preventing amount of illness.
I think in some of this discussion, people have been talking about different things.
The Israeli study with 13 times is reporting on preventing infection - i.e. above category #1. It also reported on category #5 re preventing amount of illness and we can use that to infer category #4 preventing illness if infected.
But it did NOT study or report on category #2 preventing infectionsness or category #3, preventing spread ( which is result of categories #1 and #3). Nobody has measured this directly as far as I know. You would need to do rigorous contact tracing on your test subjects and all who they come into contact with - basically impossible.
What do we really care about ? Categories #3 and #5. And NOT category #1 by itself.
Whether someone gets infected by the virus is a zero problem itself. The problem is causing illness and spread to others.
In fact early vaccines have the purpose of increasing the chance of infection to 100% by actually infecting you with a weak form of the virus. With the idea that the resulting infection will be so weak that it will itself cause little illness or spread to others. But will cause your immune system to ramp up to reduce future illness and spread.
So when I was saying for months, by comparing Rs across locations, that natural immunity was more effective than vaccine, I was talking about category #3, which is preventing spread.
The Israeli study reporting on category #1, preventing infection, only helps you by revealing one part of preventing spread, which is preventing infection. But still guessing about the other factor of preventing infectiousness.
Is it possible that the reality is that the vaccine is better than natural immunity in preventing infectiousness, even if it is worse in preventing infection and in preventing those infected from becoming ill? I suppose but hard to see a mechanism for that result.
And, going from my prior post, what is herd immunity based on ? Category #3 preventing spread. Which is the result of category #1 preventing infection combined with category #2 preventing infectiousness.
Preventing illness in the vaccine taker itself is irrelevant in herd immunity.
Jimm,
When you insist that the vaccines were not intended or expected to prevent infection, are you limiting that to my category #1 of actually reducing infection or meaning category #3, preventing spread?
If you are just trying to say that the vaccines were intended to reduce spread by preventing infectiousness and not preventing infection, I think you are wrong but the distinction does not really matter.
And the vaccine was simply intended to get the body to create a antibodies focusing on the spike protein ( taking about the mnra ones - others might mimic natural and focus on whole virus). Doing that you would always expect for it to be somewhat effective in preventing infection, preventing infectuoisness and preventing illness in those infected .
By the same mechanism.
For our purposes, an "infection " is when the virus becomes numerous to be detected by pcr test. If the covid virus manages to infect a few cells and reproduce a little but the antibodies kill it off before it can go farther, I guess technically you are infected but nobody will ever know or care so does not really count .
So viruses enter body. Antibodies start to react. If the antibodies react quickly and strongly enough to knock out the viruses before they can get established enough to be detectable, then the vaccine prevented the infection.
If the antibodies cannot work fast enough to stop the infection, then they will still fight the virus. That should eventually reduce the viral load below what it would have been with no vaccine. And reducing the viral load will be the way that the vaccine both reduces illness in those infected and reduces infectiousness and thus spread.
How would it be possible for the vaccine to reduce illness but not reduce infectiousness ? Would not the same mechanism reduce both.
I think you are getting hung up on sterilizing immunity where the vaccibe just prevents infection 99.9 % of the time- just stops the virus dead in its tracks. Yes, that is quite rare. Even natural immunity is rarely that good ( I myself got measles twice when I was young) .
But vaccines are expected to at least reduce infection somewhat. And reduce infectiousness for sure simply by the sane mechanism by which they reduce illness.
What I think is happening with delta and the current vaccine is it just reproduces so fast. With original covid, the antibodies were able to kill off the viruses before it got to infection level very often reducing infections way down. With delta, it is just too fast and gets by those initial defenses too often and causes an infection. But antibodies still good enough to eventually get a handle on it before it causes serious illness. And that also reduces infectiousness.
Read this:
Latest on coronavirus from New Scientist
Vaccine evidence: A UK study has found that protection from the Pfizer/BioNTech and Oxford/AstraZeneca vaccines wanes over time. Both vaccines provide good protection against symptomatic infections by the delta coronavirus variant, but are around 15 per cent less effective against delta than against the alpha variant. The findings also imply that vaccinated people who do get infected might be just as infectious as unvaccinated people.
Read more: https://www.newscientist.co...
Read the last sentence again slowly
I had to read it a few times myself
"Might" is not analysis.
Your link just goes to the general site and then you have to go thru a paywall. It does not go to the article.
So, without being able to see it, some studies presume to show that the viral load at first detection or maybe at peak can be the same as for unvaccinated. But the viral load still declined faster in vaccinated as you expect. If the antibodies are stopping the virus enough to prevent serious illness, it would seem they would have to at some point be reducing viral load..
So maybe just maybe the breakthrough vaccinated case can be as infectious at one point. But what we should care about is total infectiousness over life of infection
RT, if you read the links I dropped (the second set I think), which aren't that long, you wouldn't have needed to ask those questions.
Bottom line, even the real-world data from Israel shows the vaccines are highly effective at preventing severe disease, hospitalization and death, which is our primary short-term objective to prevent the collapse and overwhelming of our emergency medical systems (where even non-COVID emergency patients would be impacted, e.g. car accidents, heart attacks, strokes, etc.), and the standard to pass clinical trials was this same metric.
Preventing infections is a related but less important matter, especially if the current vaccines are effective at preventing serious illness, hospitalization and death, since the dominant variant will no longer be dangerous for high 90s% of vaccinated, which is what we want as it should burn through society at that point and not likely be replaced with more virulent variant (where's evolutionary fitness in killing hosts against dominant one that doesn't)?
That's just our society tho, we should be less interested in boosters than in getting rest of world vaccinated, as virus variant fitness parameters will be different out there, and in our globalized connected world come back to bite us in the ass. Case counts are not all that important right now aside from further showing how effective the vaccines are in comparison to blnot being vaccinated.
Ending up with a dominant endemic variant that is mostly harmless to vaccinated folks is what we should be aiming for, we're not ever knocking out COVID completely, not even in this country given our significant science-denying minority.
See I do not think we are really disagreeing on anything important. I think much of the above was maybe some talking past each other with different terms.
I do think you are maybe misremembering the history of what was intended for the vaccine and what vaccines normally do. See qx49 post above and our back and forth.
But who cares about that now. If you are wrong on that, just does not matter to me.
Because I think we basically do agree on where we are today and what we are facing .
One thing you mention is where to use the vaccine. Something that is missing in the Israeli study discussion ( I am guilty too) is what is the most important thing it shows.
We already sort of knew from real world that the vaccine was not doing spectacular at stopping the spread. It just was not going to bring the R down enough even with 100% vaccinated.
So the important thing here is not that natural immunity is much better than vaccine. It is that natural immunity works spectacularly. 19 breakthrough cases for the few months where covid spreading a lot in Israel out of over 16,000 with natural immunity alone.
So focus on how good natural immunity is, not how so so vaccine immunity is re spread. And, as you say , it still.is pretty damn good at reducing illness and death.
And since natural immunity is so good , adding in the vaccine immunity is just not that helpful. A little bit margin but what is it gonna to do . Reduce 19 infections from 19 to 10. Big deal.
So, yes, do not vaccinate anyone who had a confirmed case, at least for a year. Maybe at that point it had waned enough to do. But send the vaccines you save by not wasting them on those with natural immunity to places like Africa where they can do more good, even just for the us .
But not sure if I fully agree with your last point if I understand it. If this is endemic and I need to be vaccinated every six months for the rest of my life, with some side effects every time , no thanks.
Just give me an actual covid infection when the vaccine immunity is at full strength and let me have the better stronger natural immunity for life with maybe mild infections like a cold when it wanes enough but still strong enough to prevent serious illness.
Choice one get vaccinated with side effects every six months for life.
Choice two get vaccinated before your first covid infection so it is mild and then any subsequent infection is infrequent and mild .
Choice three never get vaccinated and decide to go ahead and take a chance of catching covid with serious illness.
Choice four manage to never catch covid while staying unvaccinated while relying on herd immunity.
Not positive yet but my assessment is that Choice 4 no longer exists with delta. And, if you are saying Choice one , I am seeing maybe that is unlikely too. It will eventually get you .Choice three is clearly stupid. So Choice two it is. Maybe I want my booster soon, get to peak vaccine immunity and then i WANT to get covid.
My recommendation would be to generously read what people actually say, not what you're seemingly looking for them to say. Did I at any point recommend taking a booster every 6 months? No. The only thing I said about boosters is we should forego them for now in favor of getting more vaccines out to rest of world (immunocompromised may be legit exception).
Also, one study does not change the game, especially when you primarily concern yourself with preventing serious disease and death. 5.4 million Israelis are fully vaccinated, and only 300 or so of that group are currently hospitalized, so only 1 in 18,000 people! That's a success story 18 months into a novel pandemic, not any reason to panic or overstate the crisis.
For all we know the current t-cell protection may last for years in preventing serious disease and death - there's no scientific reason yet for the Israelis or us to crowd back to the front of the vaccine line for boosters.
Stop incessantly and overdramatically worrying about infections, every new infection of a vaccinated person pretty much makes her/him and us stronger overall, and lessons our risk. The unvaccinated fortunately are facing unacceptable risk, and endangering our emergency medical care system along with it (not to mention costing us billions of dollars).
...unfortunately are facing unacceptable risk...
Also, the reality of the situation is kids are going back to school, and hence the virus is only going to gain more momentum in immediate period and near-future, the vaccinated will be exposed and mostly just become stronger, we shouldn't overly concern ourselves with blocking infections of them with fresh antibodies (except perhaps the health-compromised).
As for the unvaccinated, boosters don't even apply to them obviously, and those that survive this wave will likely emerge the stronger for it immunologically, and it will becomes less critical a priority to try and get them vaccinated (while at the moment this is still our most critical goal).
And kids are in the same boat as the unvaccinated mostly, boosters obviously don't apply to them, and it's mostly too late to vaccinate them for this pandemic wave, with them going back to school and not having an approved vaccine for the vast majority of them (and the public having no taste for another widespread lockdown).
Except the risk for kids being extremely low, as opposed to adult unvaccinated population, which isn't going to be comforting anymore when whatever % of them do get serious illness or worse, considering the large raw numbers of the pool, but this is something we've already failed to prevent unless we lockdown the schools again, so the best we can do is masking them up, which may or may not be effective depending on quality of ventilation in the classrooms (another preventive intervention we largely failed to make, as would take months of advance time).
Doings in Hawaii: https://abcnews.go.com/Lifestyle/wireStory/covid-19-surge-pummels-hawaii-native-population-79673153
Jimm,
I said in my last post IF I understand what you were saying in your last point . I really was not sure I was disagreeing with you or misunderstanding what you were saying. That is why I phrased it that way.
When you said we should be aiming for an endemic that is mostly harmless to vaccinated folks , that sounded like you were talking about recurring vaccinations to deal with that endemic virus. Instead of a vaccine making that first infection that gets you the natural immunity largely harmless. Or maybe you meant we should be aiming for a vaccine that can give us long term immunity as good as natural. I can agree that is even better but doubt it is attainable.
Most of the other things in your latest posts I agree with. Yes, this is just one study and not yet peer reviewed. So I am not yet jumping to any conclusions that it is right. Not until I see more discussions about it and real contrary analysis . But I do tend to look at studies that might be too technical for me to understand every detail and see if anything jumps out as not smelling right . And that " smell test " serves me well. When something seems fishy , I usually find it does get officially discredited later. And this study has easily passes the smell test so far.
Actually would not be surprised if it turns out that the 13 times better natural immunity is similar high but still a good differential. Note the CI has a decent range so reality could easily be on the low side of it.
And I am NOT one who is worrying about new infections. Same as you, I recognize they are building immunity. If we are going to get it eventually anyway if it becomes endemic, why not now ? Except for keeping it low enough to not overwhelm medical care , just let it spread now until we hit herd immunity and even after to drive R down, before winter hits. So no masks unless cases reach a level where they threaten health care capacity.
On kids, they are basically like vaccinated adults. Their risk is that low. As unvaccinated, their risk is less than annual risk from the flu . The reduction in child deaths for the almost disappearance of the flu last year is larger than child deaths from covid.
So do not tell me that masking kids, and making their precious childhood years a mini nightmare, is for THEIR benefit. It is to help the more vulnerable older folks like me . Not willing to do that. Or more precisely, it is mostly to save the lives of older adults who refuse to get vaccinated. And just not willing to make kids for them.
Look, the unvaccinated adults have had their chance. They made their bed, they have to lie in it. And continuing to make life miserable for everyone including children whose risk is extremely low , and vaccinated adults who have protected themselves, is no longer reasonable. Maybe it is tolerable to wait until we get a booster shot for those vaccinated with no natural immunity ( those should be available right now) but then I am done.
Anybody who refuses vaccination is almost surely going to get covid if they have not already had it. Nothing we can do about that.
We have to keep masking up to possibly meet the goal of keeping hospitals and emergency medical care available and high-quality to everyone, not just the unvaccinated COVID patients (as well as keeping health care works from quitting from exhaustion/despair).
Aside from that, we do not keep needing to get boosters for this to become endemic, at least not until we know more about the length of the memory t-cell protection against severe disease and death. Antibodies and infections are secondary concerns, except for the sheer numbers of the pool of children we're talking about, which will likely lead to intolerable numbers of children hospitalized or dead regardless of how small a proportion their overall risk.
But there's little we can do about that at this pandemic wave stage short of lockdown, except to at least out of an abundance of caution and the precautionary principle make sure they are masked (which in poor ventilation may not make as much difference as we hope).
The good news is that vaccine effectiveness is holding for the most important metric/criterion, with the current Delta variant which is not all that virulent to the vaccinated or children, but still very infectious, which will make it all that much harder for a more virulent variant to push this one aside, and even if it does many more people will have the strongest immunity (vaccination plus previous infection) by that time, and we don't expect any upcoming variants to have mutated to be that radically different.
The real longer-term question is going to center on the long-term t-cell immunity, not antibodies, and how well that memory immunity holds up if we eventually see another variant that brings even higher viral loads, whether this potential variant arises from other unvaccinated or vaccinated parts of the world (in one sense, the evolutionary pressure required for a variant to rise to the top may differ in largely unvaccinated populations versus largely vaccinated populations, and mixed levels in between, so nothing is predictable at this point).
I should offer this caveat, I'm mostly thinking out loud here and am not a virologist, immunologist, or medical/public health professional or expert, but have informed myself through some of the top virologists in the world, many who do not feel the science is being followed or respected properly, and then kind of just reasoning through the rest of the science as well as the evolutionary aspects as far as variant fitness and associated pressures (along with my sense that the most valuable intervention outside of vaccination is ventilation, not masks or distancing or hygiene theater, at least when taking into account all the factors behind physical health).
...beyond physical health...
...health care workers from quitting from exhaustion and despair...
Pingback: Covid-19 Deaths per Million by State, 2021 year to date. | Later On
https://www.pennmedicine.org/news/news-releases/2021/august/penn-study-details-robust-tcell-response-to-mrna-covid19-vaccines
https://www.hindustantimes.com/lifestyle/health/immune-system-has-a-backup-plan-for-waning-antibodies-says-study-101630135413932.html
https://www.statnews.com/2021/08/25/covid-19-vaccines-flirted-with-perfection-reality-more-complicated/
https://www.statnews.com/2021/08/18/health-workers-overwhelmed-covid-deaths-among-unvaccinated/
https://www.microbe.tv/twiv/twiv-797/
Sorry, I didn’t read through all the comments so if mentioned previously, I apologize.
Covid, being an infectious disease transmitted mainly via breathing, is itself unaffected with respect to its transmission by which State a person lives in. Yes, of course the policies adopted by a particular State affects transmission. However, all policies are geared to the same goal, reducing effective population density. Every method by which we protect ourselves from covid is simply a mechanism to reduce effective population density this goes from wearing a mask to having both vaccinations. Yes, there are State policies but States also vary considerably in population density, just look at the lower tail of these data. Obviously, Kevin doesn’t have all the time in the world to figure out every variable and their relative importance. Some are easy, e.g., correct for the actual population density of each State but, e.g., how effective is mask wearing in effectively reducing population density and under which situations? Having 1 or 2 vaccinations etc. ? This is one aspect of things epidemiologists do, statistical analyses and modelling. Reality and, consequently, science is complicated and all analyses of phenomena have some margin of error. All this IS being done by well trained experts but to most people the actual literature on these matters is unavailable and unintelligible which is why we assume, that directives coming out of the CDC are accurate and based upon appropriately gathered and analyzed data. There are States sabotaging this by withholding data e.g., Florida. Their apparent stupidity has a reason, withhold facts and one cannot analyze and understand what is really going on, thankfully, most Governors are not psychopaths. We can’t all be experts because we don’t all have access to the necessary information and the skills to make sense of that information - some of us understand this, but a frightening number of people simply do not.
So-
After reading through the comments and trying to make sense of many of the links I have to come to some sort of PERSONAL conclusions
A - This is still a NOVEL coronavirus. WE know more than we did 2 years ago, but still have a ways to go.
B - We, as a nation are spoiled. WE want things to remain the same. But we are being affected by the political gamesmanship being played by both parties
C - we have many people who just don't give a damn about their fellow man
Meanwhile our performance in dealing with CV-19 is so bad that the EU is considering an OFFICIAL move to ban travel FROM the U.S. after months of talking about it and not wanting to piss us off or lose the travel dollars.
How does this make us feel?
This is a medical issue NOT a political issue. It's science not freedom. It's a worldwide problem. We can not control it, we did not conceive it and we cannot cure it.
I watch this as an old man and see that other countries have better data than we do. They test more, and they vaccinate more than we do. And they are doing better with CV19 than we are
Yet, we are at the mercy of other countries who don't have vaccines for either the first or second shots for THEIR population. So new variants will come out and spread regardless of what WE DO here. In a global economy it is inevitable that this will happen, and they will spread world wide
WE have learned NOTHING, it seems
A new strain within the Delta variant?
https://inews.co.uk/news/health/boardmasters-festival-new-delta-strain-cornwall-event-1172393
{snip}
Fears are rising that a new strain of the Delta variant of Covid-19 has emerged among festival goers after an event attended by 53,000 revellers in Cornwall led to sharp spike in cases among younger people.
With this Bank Holiday weekend witnessing the highest number of music lovers flocking to festivals in 18 months, Public Health England (PHE) is understood to be investigating a possible new Delta strain that may have emerged from the Boardmasters festival in Newquay two weeks ago.
A senior official working on pandemic response in the south-west of England said many of the infections among young people in the region had been identified as coming directly from the festival in Newquay, which now has the highest rate of infection in England at more than 2,000 per 100,000 people.
The source told i: “It was traced because they can identify where it came from by genetic changes in the code.”
While it is being referred to among hospital staff in Devon and Cornwall as the “festival variant”, it is believed to be a new strain of Delta rather than an entirely new variant. Delta already has around a dozen different strains.
“It’s still the Delta variant but they can say it came from the festival, hence why it is being called the ‘festival variant’,” added the official.
The South-west peninsula now home to eight of the top ten areas in England with the highest rates of infection. The figures also show that around half of all infections in England are among those under 30, with the highest rate of infection now in the 10 to 19-year-old age bracket.
{snip}
Puts a new twist on college football games eh?
There's no such thing as a Delta "strain", so that's a strange article.
What part of this did you not understand Jimm?
"While it is being referred to among hospital staff in Devon and Cornwall as the “festival variant”, it is believed to be a new strain of Delta rather than an entirely new variant. Delta already has around a dozen different strains."
Delta is a variant, not a strain, and it does itself have variants or strains (Delta Plus is a separate variant).
https://www.virology.ws/2021/02/25/understanding-virus-isolates-variants-strains-and-more/
...it DOES NOT itself have variants or strains...
Can anyone explain this strange anomaly? There seems to be two set of death data. If you go to the site Kevin mentioned a while back:
https://ourworldindata.org/covid-deaths?country=USA~GBR~CAN~DEU~FRA
you get a 7 day rolling average of over 1000 deaths per day. And it has been above 1000 per day for over a week. If you google:
"daily covid deaths us"
you get the same numbers. But if you go to other sites that are using the CDC numbers like this:
https://covid.cdc.gov/covid-data-tracker/#trends_dailycases
or "https://www.calculatedriskblog.com/" you get a 7 day rolling average that is still below 1000 deaths per day. I've seen both numbers for a while and can't explain it.
Google and ourworldindata.org say we've had many days in the past 2 weeks with 1400-1700 deaths recorded. For the same period, the CDC says 1000-1100 deaths with their very latest number 1300. The numbers are around 300-400 different and have been for at least a few weeks. I'm very curious which is right and why there are 2 sets of death numbers.
Not sure.
I use worldometers mostly as their site loads easiest and is more user friendly .
I do know that some sites such as worldometers redistributes back to prior days when a place drops some big death number because of a backlog or changing their definition or they missed reporting some prior deaths. Others do not do this and thus a big dump distorts the number re 7 day average for a week and their averages are more herky jerky.
The info kevin used to use on his old graphs did not redistibute and so was jumping around more. Of course if you use a site like worldometers to build a historical graph, you have to keep updating past numbers when they redistribute which would be a real hassle.
I think it was in the last week when the new ny governor finally changed the official state numbers to report consistent with cdc rather than the undercounted way Cuomo had been doing it. If someplace was using those fake low ny state numbers, they might have a blip up for a week . But I thought not very many were using them anyway.
Another issue is the time each site cuts off their daily figures which means some reports can be in different days.
But, if you are seeing consistently higher numbers on some sites every day, I would think that has to be a difference in their definition of death or maybe what they include as usa ( like does Puerto Rico count).
Maybe some are trying to project excess deaths above actual confirmed deaths?
"Maybe some are trying to project excess deaths above actual confirmed deaths?"
I'm sure that's not the case.
I checked the total deaths and ourworldindata.org has 637,000 deaths and CDC has 634,000 deaths. Both are less then worldometers.info with 654,000 deaths (they include probables).
I don't know why no one else has noticed this. I recall a couple news outlets either last week or the week before talking about how we were now over 1000 deaths per day on average. So I was surprised when others said we are only at 800 or 900. So Kevin isn't the only one looking at the higher number. I don't know if the google result I mentioned is using ourworldindata.org data or both places are getting the numbers from some common source.
Vog,
I think " Novel" for covid is referring to the human immune system having no knowledge of it, not the virus knowledge that human brains have of how it works.
So, as people catch it and the immune system learns, it is becoming less " novel " every day and thus less dangerous to the community. Not sure how the vaccines fit into that definition but practically they make it less novel by giving the immune system a look at part of the virus at least.
Back in the middle ages something like the flu was not novel to Europeans even though we knew nothing about viruses . But it was novel to amerindians and dangerous to them.
But if the point was we still have lot to learn, yes.
Re Europe's travel ban, that is mostly political not scientific. Once the virus is out enough in your community so that it is well established, banning travel from other nation with a somewhat higher case count is mostly meaningless. Banning travel from the USA to France when they have 70% as many cases is sort of silly.
Except maybe to try to prevent spread of a possible variant. But then you should ban travel from everywhere as a variant has a chance of popping up in a place with fewer cases too. I think some here have argued that we should close our borders too, including from Europe, for just that purpose.
If there was any time for Europe to ban travel it was right when delta hit the uk and usa but it might not have yet been established in Europe.
And what a coincidence that they ban travel now right as summer travel season ends.