It's time for my sorta-weekly look at the COVID-19 pandemic, but this time I want to focus on something a little different. If you take a look at the case rate, the US has been doing pretty well for the past couple of months, falling from 500 per million to 200 per million. Meanwhile, countries like Germany and the Netherlands are skyrocketing, and others are increasing too, though at more normal rates.
But if you look at fatality rates, the picture is totally different. The US rate has declined to 3.5 deaths per million—which is good news—but that's still three times higher than most other European countries.
To get a better sense of this seeming paradox, we need to look at the case fatality rate, which tells us the percentage of COVID-19 cases that eventually turn into deaths. Here it is:
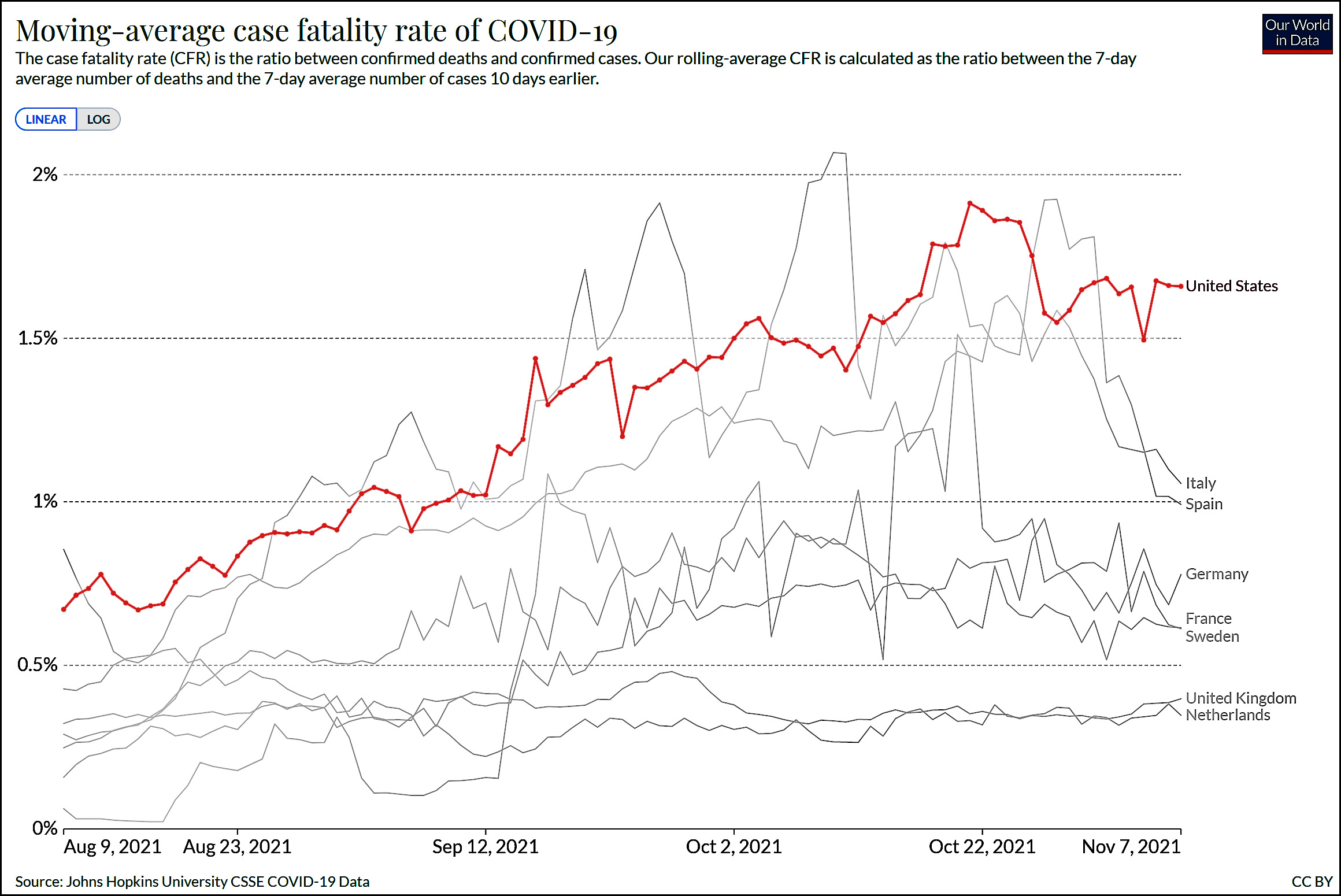 CFR is an imperfect measure, but the differences are so stark that this hardly matters. Over the past couple of months the CFR has doubled in the US and is now twice as high as in Germany and four times as high as the UK.
CFR is an imperfect measure, but the differences are so stark that this hardly matters. Over the past couple of months the CFR has doubled in the US and is now twice as high as in Germany and four times as high as the UK.
The case fatality rate tends to bounce up and down a lot, and the US rate hasn't always been higher than everyone else. Still, it's generally been pretty high, and lately it's spiked to a point pretty near its all-time peak.
Why? Why are so many more people dying of COVID-19 in the US than in other large peer countries?
Lol, Europe inflates its case count. Cut it in half. Skyrocketing it is not.
The Case-Fatality-Rate = Fatalities/Cases.
If Fatalities are too high, that makes the CFR too high. But if Cases are undercounted, that would have the same effect on CFR.
In our widely diverse country, where is the Fatality Rate high? In the Red areas. The sensible thing would be to look at the Case Rate the same way, and see if the CFR is the same, or rather does it appear that cases are being undercounted. There would surely be a motivation for that in places where denialism is rampant.
Nope. Look again. Most of what Drum is showing is a lag.
No.
Totals are higher in red areas, not explained by age.
Here:
https://twitter.com/kjhealy/status/1454430288302518276
Concur. Most other first-world countries have been tracking the hell out of their cases and busting up transmission by contact-tracing. I was in Ontario for quite a stretch of this pandemic and in the city I was in they actively monitor their sewers for genetic traces of the virus and pounce on neighborhoods where it shows up. Their threshold for an "outbreak" is a single case. Their overall covid death rate is among the lowest in the industrialized world, despite some provinces that acted much more like we do (until the delta outbreak in the fall).
In most parts of this country, on the other hand, we rely on people either self-testing and reporting, or feeling sick enough to get tested by an ER, a PCP, or a walk-in clinic and then getting reported for aggregation.
So our official statistics, in particular the denominator here of total cases, can't accurately reflect actual incidence in the same way. It would be kind of like comparing DUI figures gleaned from a roadblock sweep vs self-reported DUI numbers.
Public health is definitely stronger as a discipline in Canada (or the UK) than in much of the USA.
Not sure about places like NY City which seem to have well developed infrastructures for public health? Or Massachusetts, say? But, generally.
". . .where is the Fatality Rate high? In the Red areas."
The Red rural areas are also the areas with the poorest levels of health care. Lots of small hospitals lacking ICU's or much high cost-high tech equipment. Include a population that has a high level of preexisting conditions and a tendency to denialism that results in them staying home and taking vitamins and horse medicine instead going to the emergency room, and it is not surprising the CFR is higher.
Price of "freedom."
...and not getting the vaccine and ignoring masking requirements.
Speculation:
Political Covid deniers wait longer to get medical attention thus increasing their risk of death.
I concur. Patients in the US are sicker by the time they seek care.
Also, most are unvaccinated.
Probably because of the way American medical insurance works?
People will fear bills they cannot pay?
I think there is plenty of evidence this is true for Americans with any affliction (but less so for those recipients of Medicare b/c 1. they are insured 2. the insurance is relatively comprehensive)? Americans wait longer before seeking treatment.
Can you even buy ivermectin in Europe?
It's a very important anti-parasitic drug, worthy of a Nobel prize, so I would hazard to guess yes.
Most insurance are no longer automatically covering Covid hospitalizations now like they were earlier in the pandemic. Since Americans are more likely to be un/under-insured, perhaps more are waiting until symptoms get really serious before going to the ER, thus increasing the likelihood of serious illness and death.
I would agree that politics and lack of insurance are both playing a role.
Could it also be due to delayed spread of Delta? I just read that experts are predicting half a million deaths in the next three months in Europe.
I thought Europe was better vaxxed than the US, but that turns out not be true.
Wealthier western Europe is doing pretty good on vaxxes -- it's eastern Europe that's a concern now. Bulgaria's just over 20%, for example.
Western Europe will not hesitate to slam back down restrictions if losses get anything close to that. And indeed you have to show your vax certificate to go into any exhibition or concert in Germany, I believe.
Most major countries are at 80%+ adults with at least one shot. Portugal is at 98.5% of adults. Some resistance in France but since Macron brought in "mandates" eg you can't go to a restaurant without proving you are vaxxed, the percentages have gone up 10-120% (80s I think).
Eastern Europe is more problematic. There's much less trust of government and the healthcare system there.
I agree with the others who have suggested the health system and general health of the people getting COVID now.
As it shifted to red states, it infected more people with a) a belief it was all a hoax and they were naturally immune and thus they sought medical care later than in other cases, and b) it infected more people in states with limited health care, especially for workers.
See Dave Leonhardt's newsletter today about how much the virus has shifted red in the past few months.
Lower natural immunity as well. Case counts are outdated.
Romania has the world's highest covid death rate,
https://www.nytimes.com/2021/11/08/world/europe/romania-covid-vaccine-refusal.html
Because it's full of religious psychotics, conservatives and people made paranoid by conservatives.
No, gypsy curse.
omg, it's true!
Truth! Gotta treat the Roma better or else.
The Gypsy Traveller:
https://youtu.be/qZcrFHqQRPU
I have no idea, but I'm partial to the idea that republicans don't believe COVID is real and so just aren't getting treated. In any event...
"The brief version: The gap in Covid’s death toll between red and blue America has grown faster over the past month than at any previous point."
https://www.nytimes.com/2021/11/08/briefing/covid-death-toll-red-america.html
So... Woo-hoo! Go red team! You can't cure stupid. And really, why bother trying with this group?
Yet college educated Republicans out vax college educated Democrats, which prefer more holistic approach.
Natural immunity+vaccination, not vaccination alone in the key to understanding. The Northeast looks like the virus is mutating weaker to infect more people. making it more harmless.
Bottoms up, Shootie. After all, it's been proven alcohol kills COVID, amirite or amirite 😉
Given that 90% of Democrats are vaccinated, that sub-group of unvaxxed college educated Democrats must be pretty tiny.
Age would be a big effect?
Republicans are older. Old people are far more likely to be vaxxed than younger people. I think something like 90% of *all* Americans aged over 65 are vaxxed.
There are particular ethnic minorities, African and Hispanic Americans in particular, that have relatively low vax rates. And a lot of them are Democrats?
As if normal Republican gerrymandering isn't enough, the red states are also being apportioned and districted based on their population near the beginning of 2020, before so many deductions from the totals were made by COVID.
In the US, testing rates are low. Fewer tests given to people outside of a hospital setting will lead to a dramatically different fatality per case stat. If testing was more frequent and more available in the US, case counts would be higher and the fatality per case stat would be lower.
Widely available free testing kits = bigger numbers, faster treatment, less transmission, fewer dead people.
The partisan gap in Covid’s death toll has grown faster over the past month than at any previous point,
https://www.nytimes.com/2021/11/08/briefing/covid-death-toll-red-america.html
Again. This distortion is the northeast, which leads the country in natural immunity. Notice Florida following its "southern brothers" despite being the most vaxxed by a mile. NYtimes kisses on it again.
In order to get 'natural immunity' you have to get covid in the first place.
Similarly, all those people who have lived through a war are always talking about how it wasn't all that hazardous.
Or use Qaron Rodgers's homeopathic medicine.
It's like these freaks are playing Russian roulette with other people's heads and bragging about it.
Given Qaron is the son of a Chico, CA, chiropractor & is now engaged to one of Bernie's celebrity attaches, it seems he is getting the woo-woo alternative medicine preferencing from both ends of the horseshoe.
Natural immunity?
Is there anywhere in America where more than 10% of the population was, pre vaccination, exposed to Covid-19 infection?
Even when the UK was losing nearly 2000/day to Covid-19 (last Feb-March) I don't think there were suggestions that more than 10% had had exposure?
I have not looked at the data in detail and can't give an answer, but the first place to look is at nursing homes and other places where the elderly live and are treated. Most covid fatalities are among the elderly. You can't expect little-regulated, for-profit nursing homes to fully prepare for epidemics.
How do the charts look for people over 65?
Based on other countries, at least, the majority of Covid-19 deaths are under 65 (as are the vast majority of cases).
You can get unlucky. Very old people may have immunities that don't stick or other compromising conditions that make Covid-19 infection fatal.
But Covid is, in the developed world, increasingly a (fatal) disease of the under 65s. Either those who are immune suppressed in some way (eg cancer patients) or not fully vaxxed, or just dang unlucky.
EU scientists reveal long-term brain damage caused by Covid,
https://www.rfi.fr/en/france/20211022-eu-research-reveals-long-term-brain-damage-caused-by-covid
Less than 1%......
And 1% of your brain is all you need, as you're always happy to demonstrate.
Please don't feed the troll.
Another possible contributor here is that since the delta outbreak in the fall, hospitalizations have been happening in smaller-town and more rural areas that don't have a whole lot of bed space or ICU capacity. Only a few weeks ago several states were either triaging or about to because of overload. These patients were sicker coming in, were overwhelmingly unvaxxed, and were in facilities where available equipment, standard of care, and experience might not have been up to what they'd get in big-city centers or teaching hospitals.
Especially outside the major centers, we have very, very little surge capacity in our hospitals. There are a lot of reasons for that, but the result is that almost any significant departure from average case loads can set off a crisis.
Pingback: Is the US bad at treating COVID-19 cases? | Later On
If only Debbie Wasserman-Schultz & the Institutional Democrat Party hadn't rigged 2016 against Bernie. Then, Bernie defeats Trump & stands up Medicare4All in time to defeat COVID even before it turns pandemical.
I'm assuming that comment is serious; if I'm wrong, disregard the following.
Countries with universal health care have also had issues with covid.
Does the term "beating a dead horse" mean anything to you? What about words like "obsession," "maniacal," or "consumed"?
How about, "give it up already"?
I am still not over no difference between Gush n' Bore.
I think a major problem here is that if you try to search for information regarding the question of natural immunity vs vaccine immunity the vast majority of the results returned from search engines appear to be wingnut websites trying promote natural immunity by any twisted inference they can contrive.
'Natural immunity' is like trying to break through a wall by sitting around and waiting for birds to randomly crash into it, wearing it away in time, as opposed to using a stick of dynamite, which conservatives are confident will never work.
+1
obesity!
Testing! You test more, you get more cases!
First , the chart is off imo because of the differential lag in cases and deaths.
It uses a 10 day lag per the note at the bottom . First , in my understanding, the average time it takes to die from infection to death ( if you do die) is somewhat more than 10 days i think. But not by that much I guess and not really positive so do not want to make a big point there. I am guessing that maybe 10 days is maybe average from confirmation of the case to actual death, but that does not take into account the gap between actual infection and confirming it.
But bigger issue is the lag between actual death and reported death is is a lot greater ( and somewhat more variable) than the lag between actual infection and a reported confirmed case .
A better graph might have a longer lag time between reported cases and reported deaths - maybe an average of more like three weeks . Or best would actually be a variable lag , where you would compare reported deaths to z% of reported cases from 5 days ago , y% from 6 days ago ... a% from 2 months ago , with maybe an average of something like 3 weeks.
I noticed a while ago that a standard gap of any length does not really work exactly when case numbers are changing quickly.
This explains some of the differential of the us cfr being higher given the period shown in the graph , but I doubt most . But I do think it explains most of the unbelievable changes in cfr .
Because the 10 day lag is wau too short, you will see cfr expressed this way tend to be understated and falling when cases are rising from a lower level. Which you can see recently in Spain and Italy. But the period shown is not a period where us cases were rising fast and thus you do not see such a biased low cfr for us . In periods where cases are falling, the too short lag will bias cfr too high . And I think that is true for much of the period of this chart . Except at the beginning.
And c'mon. Does anyone really believe it is possible that covid fatality rates in reality nearly tripled over that period, while not doing so in other nations? That is ridiculous and no rational reason why it would be so. Therefore, of course your first thought should be that there likely is a flaw in your measurement, and there is here.
Ignirnt troll gotta roll. Why don't any of our resident trolls have STEM training?
Funny how you cannot actually come up with any actual logical argument with all your presumed ( and likely imaginary) stem knowledge.
You're here to be contrary. That's it. So I just remind everyone of who and what you are and from time to time kick you in the slats. That's it. As for your 'thoughts'? You remind me of Alexander Abian, Archimedes Plutonium et. al. from back in the day: It is absolutely imperitive that in every way and in every context they tell people that Einstein! Is! Wrong! Not even worth the bother of replying, really, except to tell them to shut up and go away.
But, as I said before, it is the case that the USA cfr has been higher recently, or seems to be , even if you take into account a more reasonable lag. I have said that before, especially in comparison to the uk.
Why is that ?
As others here have said, it might be partially due to differences in testing policy, rates and criteria for counting a covid death . Note you cannot just look at what % of covid infections you pick up through testing, but also what % of covid deaths you pick up ( including maybe over 100% if you are overstating covid deaths). A high cfr will tend to be the result of testing that picks up a low % of infections. But also if you pick up a high % of covid deaths, or exaggerate them .
Us policy and testing as compared to uk clearly picks up a lower % age of infections ( the uk are testing madmen ) . That is likely also true re continental Europe but not because of testing volume ( us compares favorable there) but because they have been concentrating more on contact tracing than mass random testing, which is obviously going to find more actual infections per test .
On the other side , pretty much all developed nations are routinely testing anyone who gets seriously ill with covid symptoms now . So very few actual covid deaths are now being missed anywhere ( which was not true in early days). And the us seems to have a perhaps somewhat less restrictive definition for what counts as a covid death which might very marginally bias our cfr higher ( or theirs lower) but death counting differences are minor compared to cases .
And I would note that, to some extent in most examples, " blue " states have also been testing more and picking up a higher % of infections than " red" states. Which would mean that " red" states reported infections might be somewhat understated relatively, but then of course their cfr would have to be overstated by definition.
And, finally , if you could somehow correct for the incorrect lag and testing differences, would the USA still have a higher ifr ( infection fatality rate not reported case fatality rate ) ?
I think so but hard to tell for sure .
But biggest factor not mentioned so far is WHO we vaccinated, not total vaccinations. With respect to ifr , vaccinating the young has almost a negligible effect , they just so rarely die of covid anyway ( yes, vaccinating the young can lower the total cases, including among old , and thus reduce total deaths, but irrelevant for ifr) . For ifr , the issue is almost all re what % of elderly are vaccinated. And there the USA left a significantly higher number of unvaccinated elderly vulnerable than Europe. The issue here is not total vaccination but elderly vaccination.
I think rational's general point of the crumminess of the data is solid. The U.S. has never done enough testing and I suspect it's even worse now. I also know even in the best of times the lag between reported deaths and when the actual deaths has had severe variations (the average median time has been 20 days but my understanding is that median moves all over the place...and you have up to 25% of the deaths taking several months to get reported). My suspicion is that many states aren't trying as hard in 2021 as they were in 2020 to get things right.
So I suspect between the just not accurately capturing the total cases and the possible mismatches between case report lag and death report lag makes calculating a death per case ratio at any given time a dubious proposition. (which doesn't necessarily mean more people per case aren't dying in the U.S. in other countries, it just means I am not sure the data is good enough to make reliable comparisons).
I do not think it is true that the us has not done " enough " testing, at least compared to most nations.
Our tests per capita are way higher than Germany ( more than double) and higher than Italy Spain and Canada, while just a bit lower than France and yes way way lower than the uk .
I keep hearing people say the USA does not have enough testing as compared to other developed nations without looking at actual facts. Just has not been true .
But I expect that some of those nations like Germany may have had more efficient testing in finding infections, by doing contact tracing. And, honestly, cultural differences in obedience to authority makes that more viable in places like Germany.
As I asked our Swedish friend, I do not know if Europe is different than usa in delay in reporting death . But yes , our reporting there is just too inconsistent to really be able to draw many conclusions with the analysis kevin is trying to make . I would also note that the lag in death reporting increases when deaths increase and systems get overwhelmed, pushing some of the final death reports out into a period when cases are going down fast.
If you look at action death reports by date of death from the winter wave in places it is available ( and those should be near final by now I hope) you will see a reality that is different than what it looked at the time ( and still does if you just look at report dates ) .
The curve of actual deaths by date was steeper and reached a higher peak than we thought in the winter wave , and dropped off more rapidly than we thought.
And yes , I definitely see reporting getting worse as time goes on , at least with respect to not reporting on holidays and weekends. More and more states and counties just give no numbers on weekends
And holiday distortions take forever to unwind.
How people vote for Republicans,
This guy I know, Zits, everybody calls him Zits, 'cause he's got pizza face, his uncle just retired after forty years at the canning factory so he sits around all day looking at stuff on the computer and he sees all kinds of shit you wouldn't believe.
No curiosity and even less imagination. That, BTW, is the fundamental problem, not that conservatives don't have empathy. They do, but the bad stuff has got to literally walk up and clobber them and theirs before they'll cop to the fact that something's going on here.
COVID proteins that trigger strokes and heart attacks identified by Israeli team,
https://www.timesofisrael.com/covid-pieces-that-trigger-strokes-and-heart-attacks-identified-by-israeli-team/?utm_source=dlvr.it&utm_medium=twitter
I am not a “number and charts” person, as Mr Drum is but I guess Mr Drum is comparing apples and oranges again.
During the pandemic has media ,vigorously and insistently , been running some kind of “world cup” in Covid death statistics on a daily basis not caring that no countries has been reporting in a similar way.
Comparing in this way is de facto trying to do a multi center study but totally disregarding all rules that is set up to do such a study in a proper way.
This is a short definition:
A clinical trial conducted that follows a single protocol but is conducted in more than one place and, consequently, by more than one investigator.
These charts presented in this article is also breaking all rules
Greetings and good night from your Swedish friend
Maybe you have some info from Europe on one thing . What is a realistic gap between reported cases and reported deaths in Europe? I have some knowledge on that with usa and know that often it takes a long time for deaths to be officially reported here. But is that less true in Europe? Maybe there a 10 day lag from Kevin's chart for presumed cfr is more realistic, which should reduce the big understanding or overstating cfr due to incorrect lag.
At least for uk, any incorrect lag bias should not be much of a factor in any case as their case numbers have been eerily flat for months . And we see their cfr in the chart stating fairly stable.
That’s an almost impossible question to answer. Remember, Europe consists of 49 independent nations. Many Americans believes Europe is the same as EU and EU is some kind of “the United States of Europe “ .. we aren’t
I am sure you are an intelligent well informed person who knows better but it’s an impossible question
It totally depends upon country. UK the reporting is pretty prompt (perhaps 1 week delay) but there is a noticeable wobble at weekends (and then an increase Monday-Tuesday as things catch up). Bank Holidays also.
I would think 2 weeks is pretty reasonable for any Western European country. Not sure about Eastern Europe.
I guess I'll post this link once again, sorry to all of you who have already seen it so many times... but it seems it may still be of interest. This shows the death report delays together with actual dates of death in Sweden, from the first wave until today.
https://adamaltmejd.se/covid/
I would be very interested if anyone has similar info from other countries.
Also have a personal question.
Whether you agree or not , I tend to think that maybe you need to get covid and natural immunity, supplemented by vaccine immunity, to get good long term immunity. Plus appears that covid will be endemic enough that almost hopeless to expect that you will never get covid even if vaccinated. And I expect the real death risk is from the first time you actually get covid and your body has to deal with the virus , with vaccination helping but not super.
So that would lead to best strategy being to
GET covid when your vaccine immunity is at its peak and your death risk from getting it first time is the lowest.
I am now two weeks from vaccine booster so should have leak immunity from vaccine. So should I hope to get a breakthrough case and try to get exposed now ? Asked only partially facetiously.
But here is real question. Assuming for now you want that strategy, how do you know you have been infected ? If you get infected while at peak vaccine immunity, good chance of zero or mild symptoms so will not know. Do I want to get tested every week ? No. And if the vaccine beats it quick, weekly testing might not pick it up. If I got infected and did not know it , so have best hybrid immunity but do not know it , I will be just as worried in 6 months assuming my immunity is disappearing.
Plus , I wonder if to get truly effective natural immunity, you actually have to get significantly sick so your immune system takes it seriously.
Maybe the vaccine, at peak immunity, prevents serious illness but , by the same token, prevents solid natural immunity from developing. So catch 22 and just eventually have to get sick from covid at least once. Aargh !!! No way out .
And in antibody blood testing, do they differentiate between vaccine antibodies and natural? If I got a blood test in 3 months, would it tell if antibodies are just vaccine or I had a breakthrough infection?
Human contact with this virus is a completely new thing in the world as of about two years ago. The one really big thing we don't know about it, because it's something we can't know, is how it might affect us months and years after we contract it in whatever degree. So within reasonable bounds, doing what we reasonably can to avoid contracting it seems pretty rational to me.
So far, with the delta variant that emerged this summer, it's been extremely contagious and at this stage seems to have killed somewhere between 1 and 3 people in every thousand (overwhelmingly among unvaxxed) who are known to have contracted it. There are some regularities in there-- the known co-morbidities-- but it also seems very capricious in its effects because some people barely have sniffles while others have barely escaped with their lives and many are living with significant aftereffects.
Given that, in these early stages of human contact with the virus I have zero intention of deliberately contracting it. As it continues to spread and mutate, it may become less lethal-- a lot of researchers were saying this about a year ago (because that seems to have been the natural history of the coronaviruses that cause common colds now). On the other hand, it may not. Nobody knows. Everything is a guess.
This virus appears to work by binding with ace2 receptors, which are found all throughout the vascular system (and I think in lungs, because ace2 is very active in them); a year and a half ago in its early stages I remember seeing that front-line doctors started to say you have to think of this as a vascular disease rather than a lung disease, and the Israeli research above echoes that view. That means it can be active just about anywhere you have blood vessels.
The mrna vaccines were designed specifically to develop immune responses to key proteins on the binding structures. These proteins and structures may mutate, to be sure. If they do, though, they may no longer bind to ace2 receptors and thus end up neutralizing the virus, or they may change it to cause a different kind of disease acting by a different mechanism.
I don't know what elements of the virus our natural immune responses act on. I also think we don't know whether a natural immune response will destroy the virus, or just suppress it. As we know, chicken pox's virus isn't destroyed by the natural immune response, but becomes latent and can emerge much later as shingles. Chicken pox is caused by a different kind of virus, one that's stable, but the point remains. Natural immunity does not always destroy what it develops against, but reaches a modus vivendi with it.
Given all this, my humble opinion is that any unvaxxed person who would deliberately get exposed to any variant is crazy-- playing Russian roulette with at least 3 live bullets in the ammo belt's thousand rounds, and a lot more in there if they have Dennis Praeger's profile. And if they survive as most do, they'll then be experimenting on themselves with the unknown consequences of having contracted a disease agent that we know nothing about over the long term, because we can't know, because it's new in human experience.
It's different for vaxxed people like you and me, of course. Ymmv, but I have no problem following reasonable steps that will minimize the chance of contracting this virus casually. But then it's easy for me because I don't particularly care for hanging out with big noisy crowds. Movies or concerts maybe, depending on local behavior patterns and transmission rates and stuff like that (in the current state of the disease).
I also don't see any advantage in trying to provoke a natural response, because there's no telling whether it would be even *as* effective as a vax response over the long term, let alone "better" in some way. It might be, but not necessarily; look at chicken pox. Ymmv here too.
Main thing for me is that it's very, very early days in terms of our experience with this virus, so to the extent that infection by it is reasonably avoidable, I think it's worth taking reasonable steps to avoid. If it becomes endemic then eventually I'll probably contract it like everybody else and there's nothing to be done about it. But that would be the definition of unavoidable.
Also to add that everything I've said above is from a purely selfish point of view and takes no account of the moral or utilitarian case for minimizing the chance of transmitting this virus to others who may, or positively don't, have any defenses.
When covid first appeared in the spring of 2020 I was going into a retirement home every day and lived with the resolve not to be the vector that brought it in. How could you live with yourself if you did? Of course if I were to show up there now they would all be vaxxed. But a lot of people out there among the general public are still more vulnerable than most, and except for kids under 5 you can't tell who they are just by looking. I think there's still some responsibility on the rest of us to contain the chance of exposing them.
The assumption that getting Covid conveys good long term immunity is suspect.
There are plenty of viruses where that is not the case. Indeed some (measles) actually reset your immunity to an earlier (less immune) state. Quite a nice trick for a virus reproductive strategy!
Humans, Covid-19 & evolution have quite a lot of work to do together, yet.
Indeed for flu we start that cycle anew each winter.
It *is* true that if you have had Astra Zeneca (or J&J) as your first immunization, you appear to get a much superior immune response with a Pfizer or Moderna booster.
It also helps if you had a long gap between first and second AZ shots (12 weeks+ seems to be optimum).
How come the ratio for the U.S. is so much higher now than it was at the end of July? you might just as well ask.
The least plausible obvious answer is that treatment has gotten less effective.
A more plausible answer is that cases are more heavily concentrated among older Americans now than in July.
But I believe two other effects are to blame. One is that the fraction of cases that go unconfirmed varies a lot from month to month, and that it is higher now than in July. The other is that a 10-day lag (as used in the plot) is too short, which means you'll get an artificially high ratio when cases are falling and an artificially low ratio when cases are rising.
I see no reason to think cases are now more concentrated among the elderly now than in July. And really it should be unvaccinated elderly. And I would expect that , as the last wave ate up and infected those most vulnerable, and you got a higher % age of breakthrough cases as immunity waned, that the % of infections that are unvaccinated elderly should have decreased. So seems implausible to me .
And I also see no reason to believe that the %age of cases we are picking up has declined in any significant way from July. Why should it have?
But, as I said above and you agree , a 10 day lag is just off and distorting.
Thanks, Rational Thought, for giving your view. The lag problem is the clearest part of this.
However, even using what I think is a better lag, of 21 days, I've seen a lot of CFR variation this year, mainly in June and July, when it was over 2% in the data I was studying. (Lately it's been close to 1% again.) I see much less variation in fatalities per hospital admission. That makes sense to me when I suppose that hospital admissions are well reported and are being done according to fairly steady medical criteria.
The efficiency of case detection, on the other hand, really depends on who's getting tested, which I think is open to big swings based on time of year as well as policies chosen and modified from time to time by governments, schools, care institutions, and businesses. It also depends on the level of covid anxiety. When death rates get relatively low, people don't worry and don't get tested as much. I think testing fell off particularly in June, after the school year ended and when death tallies were relatively low.
Re the 21 day average lag , that might be an average assuming that the actual deaths are evenly spread during the prior period.
But what if they are not?
Assume that deaths are 20% of deaths lag cases by a week. 20% by 2 weeks, 20% by 3 , 20% by 4 and 20% by 5. Consistently.
If there were, in reality , zero deaths over more than a week ago , 100% of deaths reported would have a one week lag . If zero deaths after a month ago , all reported deaths would have a 5 week lag. If equal deaths each week , average lag is 3 weeks.
The distribution of deaths in prior periods - the shape of that curve - might not change the % reported per time period, but it changes the average lag .
Back in late spring when actual cases and deaths had almost disappeared ( before delta hit) , a huge part of the deaths being currently reported were from months ago during the huge winter wave . It was not that the % of those earlier deaths that were badly delayed was so high . It was just that a small fraction of real high deaths thar happened in January was a big number compared to a high fraction of deaths that happened a week ago because there were so few.
Back in late spring, the cfr using just a 3 week lag could look insanely high. And, when the delta wave was in full swing and just 3 or 4 weeks old, you got too low a cfr with a 3 week lag because the reported deaths were including nearly zero old delayed deaths.
I do agree with much of your characterization of timing of testing changes . But it is not consistent with your earlier possible explanation of cfr going up because of lower testing in later period in the graph. The earlier part of the graph was a period of lower testing than the later part. Some because of school reopening, some because of alternatives to vaccine mandates , and some poorly timed public reaction.
The reaction of the public to the covid waves has been sadly laughable in timing.
The various covid waves hit harder and faster and went down faster than we perceived due to lag distortions. And the lag itself meant that the timing of the wave was perceived as later than reality too. And this was exacerbated by the stupid focus on number of deaths reported per day , when they are actual deaths scattered months back .
And the public tended to react to finally perceiving a covid wave by some finally getting vaccinated and being more serious in restrictions like masking.
But , in general, by the time the public reaction to the perceived covid wave by noticing the deaths , the wave was already in rapid retreat and the risk diminishing. Especially for vaccinations as you need around 5 weeks from first shot to get good immunity.
If you are going to wait until you see reported deaths rise to adjust your behavior, that is way too late .
And people also stay scared too excessively after a wave has passed but the reported deaths are still coming in.
Whoa. There's a lot to digest there.
On one point, it would be simpler to construct a meaningful case fatality rate if every reported death exactly lagged that case's confirmation report by the same amount every time, and of course that's not true, so it's all only rough estimation. I don't know what to say about the timing effects you're suggesting. I don't think there was much effect from months-delayed death reports, though.
On a second point, I should not have suggested that low testing activity in October was a likely explanation for the plotted CFR peak in October. It was just one plausible idea off the top of my head, but the motivation for it disappears when I look at computed rates with a 21-day lag, where there is little movement in CFR after August. That swelling up in September and October in Kevin's chart from OurWorldInData.org is mostly caused by the bad guess on the lag time.
I do apologize because I did think it was clear that you only meant when you brought up testing rates changing, that you mentioned it as just a more plausible possibility to consider, not that you were saying it was when looking at evidence.
I thought I had made that clear in my post and I was just saying that , looking at evidence, that plausible possibility looks wrong. I did not want to imply that YOU were wrong in raising that as a possibility.
I do not think you ever said it was likely , just a plausible possibility to test based on evidence ( i.e. plausible before looking at evidence).
There is nothing at all wrong there with what you said initially..
All right. I'm not always clear, but you understood me well anyway.
On testing differences, assume that real ifr is .25% everywhere and everyone the same.
One extreme nation A has massive random testing that picks up just under 50% of all infections and also tests anyone who is hospitalized and dies. So actually picks up exactly 50% of infections and 100% of deaths and cfr is .5%.
Nation B random tests 50% of the nation totally randomly and nothing else . So picks up 50% of infections and 50 % of deaths and cfr is exact ifr of .25%. They get cfr " accurate " but still stupid policy.
Nation C tests anyone who gets very sick which is 10% of total infections and does inefficient random testing which gets another 15% . They get 25% of infections and 100% of deaths and cfr is .1.0%.
Nation D does effective contact tracing plus tests those very sick . Thus , while doing less overall testing, the contact tracing gets a lot of non sick cases and they end up getting 50% of infections and 100% of deaths. And get a cfr of .5%.
Nation A is uk, nation C is usa, nation D is Germany.
Less testing in the US could easily account for almost all the discrepancy, right?
Cumulatively, (ie, since February 2020) the country's testing numbers don't look bad. But if the US has fallen behind other high income countries with respect to testing in 2021, it may be that we're simply identifying far fewer covid infections than many other developed nations.
If that's the case, the case fatality rate in the US is going to look a lot worse, because a lot of covid infections in the US aren't identified until a person is sick enough to show up at the hospital (and plenty of such patients, unfortunately, die). And yes, add to this lack of insurance, more obesity, the effects of poverty and so on.
But for my money Occam's Razor suggests the issue is lagging test capacity compared to other rich counties.
And yes, this would also imply covid itself is more widespread in the US, and possibly more deadly, too.
I think your are contradicting your own point . At least it sounds that way .
From your prior post , yes , less testing picking up less cases would imply that we have more cases compared to the other nations. Of course. But it by definition would also mean it is LESS deadly, not more . At least if you mean compared to what the cfr presumably shows compared to other nations.
So I assume you mean you think it is more deadly re absolute deaths, not deadly as in per infection. So more deadly than we think due to more infections and not a higher chance per infection, right ?
But I doubt that is an issue except infinitesimally now . Testing issues really only matter for how many asymptomatic or mild cases we pick up. It really is not an issue re those who actually die. Pretty any person who checks into the hospital now gets tested, even for something unrelated, just for safety of others. How do you see a real life scenario where someone actually catches covid , gets sick and dies from it, and never gets tested due to lack of usa testing supply or policy.
Now, say compared to the uk ( which I think has a comparable covid death definition), it might be true that their higher testing rates will cause a false covid death to be counted but not likely the other way .
In reality though, I think your main point is that the graph kevin shows, to the extent it still does show a higher usa cfr if correctly lag adjusted, probably demonstrates more that there are higher usa case counts relatively instead of a higher usa cfr .
But not due to volume of testing. No, we are not higher than places like Germany because of just a higher testing rate in prior periods and they are higher now. Their cumulative testing per capita is not catching up - they have always tested less absolutely. But their fewer tests are more efficient than here .
For example, those who were not vaccinated because they had and recovered from covid recently sometimes had to be tested weekly at their jobs. Which is a waste as very rare to catch covid soon after recovering ( wait 6 months and maybe different).
With Canada, not sure if their correct testing rates are thar much lower ad they do seem to have caught up on cumulative as a ratio.
Uk current testing rate probably even greater comparatively than cumulative. Last year they were at one point behind us..
And I would like to believe in a way that we have missed way more cases than Europe. As that would imply that more have natural and hybrid immunity and not many left vulnerable to infect. So we would be done with real pandemic and into milder endemic phase. But the evidence in case trends just do not support that . I think we have one more small wave this year to contend with in mostly northern blue states where there are less previously infected. Note that ny and NJ still holding up pretty well, when biggest advantage they have is high natural immunity from well over a year ago , is hopeful long term .
I think fla and many southern states are done with waves and into endemic stage . But looks to me like endemic might be as much as maybe one case per 10,000 every day on average for years.
yes , less testing picking up less cases would imply that we have more cases compared to the other nations.
No, the testing situation alone would merely imply that the US identifies a smaller percentage of covid infections. As an isolated datapoint, it says nothing about how much covid "we have." What implies we have more covid is: more Americans are dying of covid than denizens of other high income countries.
But it by definition would also mean it is LESS deadly, not more.
Not so. More Americans are dying of *covid. That's means covid19 is possibly more deadly (ie, US healthcare is less effective at preventing covid deaths). It also possibly means the US just has more covid. Or (my guess) a combination of the two. I used the modifier "possibly" in my original comment on purpose.
Not sure about your inferences, by my guess is:
A) The covid virus is indeed somewhat more widespread in the United States than in most high income countries (although the gap may well have narrowed in recent weeks; by all accounts Europe seems to be catching hell), so, all things equal, we'd expect that more Americans are dying (and have died) of covid than is typical of the rich country average;
B) But things aren't equal, though, for a variety of reasons— (lagging vaccine rate, more poverty/obesity, greater resistance to masking; high uninsured rate)—which tends to make covid19 somewhat more deadly in the United States than Western Europe, Canada etc (under this scenario, such factors would outweigh the country's modestly younger age skew).
C) In addition, the US testing rate has lagged in recent months (perhaps through much of 2021?) compared to other wealthy countries, which boosts the reported case fatality rate (I believe the US was doing ok on this score, comparatively speaking, in 2020).
Again, this is what to me appears to be happening, but it's obviously hard to tell, and reliable testing statistics in particular strike me as being difficult to obtain.
Testing issues really only matter for how many asymptomatic or mild cases we pick up
Yes, of course. If we don't "pick up" as many asymptomatic or mild cases as other high income countries, our reported infections totals will be inaccurately undercounted, which will obviously have the effect of artificially boosting the case fatality rate.
*It's been a while since I've looked at the general mortality statistics, but IIRC the data strongly suggest that, here, too, the US is performing badly; that is, while all countries undoubtedly have seen significant death-by-undiagnosed covid, we've seen more than the rich country average.
Seems most of our disagreement is semantic and not real .
When I said less testing picking up fewer cases implies we have more cases than other nations, I meant vs what the case counts would appear to show. I thought that qualification was implicit in what we were discussing. Of course it implies no such thing as an isolated data point.
On deadly , if you read what I said, I explicitly stated I was talking about " deadly " as in the chance of dying if infected , not deadly as in total deaths which also factor in chance of getting infected due to how prevalent it is . In the context of this post re cfr , obviously that fits the context. If you read my post fully, you could see I was speculating re what you must have meant which was different, which I thought was that there were more deaths than the death numbers indicate. But if just trying to say less testing caused more total deaths, presumably because it did not help to control the spread and thus caused more infections, well maybe but seems not too relevant re discussing different cfr.
Some of Europe like Germany has not just caught up with the USA in confirmed cases per capita, it has passed us by in the last two weeks ( but not France ). Germany is threatening to actually pass us in absolute cases per day ( they just went over their peak cases from their winter wave ). The uk has had more cases per capita for months, and by a good margin .
Part of that might be us picking up a lower percentage, but not all. Clearly uk has to have had more actual infections and Germany has to be at least equal to us now . There is only so many untested real infections there could be before you get just too high a % age of total infected to be believable.
I still greatly doubt there are huge differences in the ifr caused by medical care between developed nations and doubt greatly usa is neat bottom there ( I guess Italy). Our medical system is more expensive partly because we have more excess capacity which helps in a crisis. And no way I believe the uk is better there. Re obesity and overall health, we are worse to some extent but not that much. And not much different than uk. Things like restrictions and masking theoretically make a difference re total community spread and prevalence ( we can argue how much) but not really much for ifr which is the issue here. Basically irrelevant.
I think you and others keep conflating the idea of total deaths ( which includes differentials in spread rate and prevalence) with the cfr or ifr which is the chance of dying if infected, not chance per capita.
And it is remarkable how close many nations are , seemingly converging near the same figure , even with such different policies. Cumulative deaths per capita are pretty close re usa and uk and France and Italy not far behind. And note that total deaths per capita in places like Italy, France, NY, NJ are likely biased lower as they had their worst wave with initial spring 2020 - when lack of testing and chaos meant a high percentage of actual deaths were missed. Factor that in and possibly all those nations are really almost same total deaths. Germany still clearly lower but looks like they may catch up some now .
Just seems that, in the end , maybe delta is just going to have to infect a certain % age before dying down. Cannot stop it and masking and restrictions just delay the inevitable. Note that delaying that while waiting for a vaccine ( to lower ifr ) made sense. Now not so much.
Biggest factor that was somewhat in our control in preventing total deaths to me will not be any lack of covid restrictions and masking which will make almost no difference in the end. Or total vaccination rate . But vaccination rate among elderly, those who are the bulk of deaths..that really is the biggest difference. And our vaccination policy to give 2 shots in 3 weeks going through group by group ( and not strictly by age ) clearly to me was inferior to what they did in Canada.
I have trouble understanding why those like you who seem to want to exaggerate how relatively badly the usa did keep referring to Europe much . The comparative arguments there are weak. Harp on Canada, they are the relative success that make us look bad . I sort of thought that they could pass us by as winter hits there earlier. But so far they are holding pretty low .
I have trouble understanding why those like you who seem to want to exaggerate how relatively badly the usa did keep referring to Europe much
I have zero desire to exaggerate anything. The fact remains the US has lost more people to covid, proportionally, than any other large high income country (and most small ones). And, the gap in performance between the US and such countries has mostly widened over the course of 2021. The seven day death/million number is currently about 25% worse in the US than the UK. About double what it is Germany. And about 4x-5x worse than Italy, France or Spain. And that's to say nothing of America's more serious problem with vaccine hesitancy...
I could mention that the us 7 day death rate as of yesterday is less than 22.5% of the uk number . So why did you state it as about 25% , rather than about 20% or give exact ? A little exaggeration there. But that small exaggeration is petty and I have no problem at all with the description for other nations. So how about if I say you want to " emphasize " where the USA looks bad rather than " exaggerate ".
You could mention that it is not all that clear that nations like uk. France , Italy and Spain really have lower cumulative death rates given different policies on counting, and higher missing deaths early on ( where European deaths are more concentrated). But you do not mention that . Incidentally my guess is that uk is a smidgen below usa in reality but close. France almost surely below some. But I think Italy higher in reality.
And you do not mention that the USA death rate has been dropping while Europe had been rising. And that should continue given what we know the recent trends in cases have been . If last week's change continued one more week at same rate,
Comment cut off.
Saying that if same trends continue just one more week at same rate , both uk and Germany will have higher 7 day average case rates than usa, but very very close.
Since there is a reporting delay , your point of wanting to look at just current rates and not cumulative may already not make usa look bad .
Because they are idiots who think it is just the flu until they can't breathe at all?
Just a guess.