
This is insane:
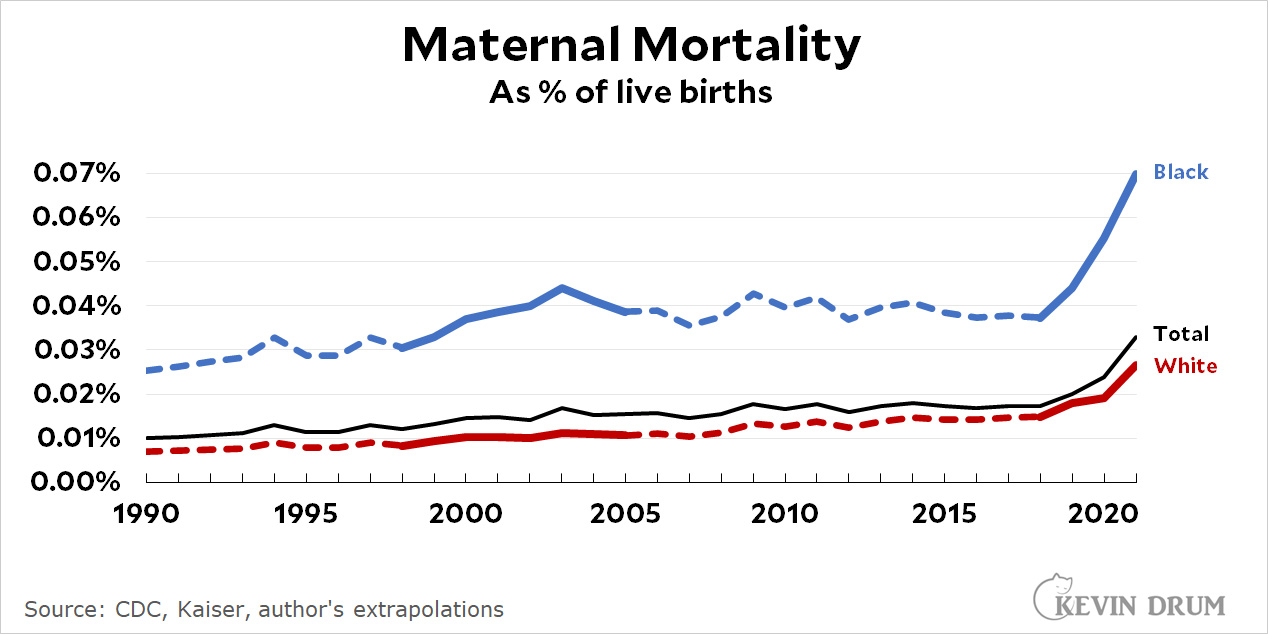 It's insane that maternal mortality has gone up 3x since 1990. It's insane that it increased 40% in 2021 according to the latest data from the CDC. 40%! It's insane that Black women have a maternal mortality rate 170% higher than white women.
It's insane that maternal mortality has gone up 3x since 1990. It's insane that it increased 40% in 2021 according to the latest data from the CDC. 40%! It's insane that Black women have a maternal mortality rate 170% higher than white women.
Something seriously doesn't make sense about these numbers. Why would the overall number increase 3x during a period of improving health care? Why would the rate for Black women be stable for 15 years and then suddenly skyrocket starting in 2019? Why is the Black/white discrepancy so stubbornly high?
It's not because nobody cares about this. It's getting more study now, but researchers have been trying to puzzle it out for a long time. Nor is the racial gap due to racism—not entirely, anyway. Nor is this upward trend happening in other rich countries. Only in the US. And we've been pulling away from other countries only since 1999.
There are lots of theories about this, but none seem to match the data very well. And none of them come close to explaining the explosion of maternal mortality starting in 2019. Even the 2021 increase is mysterious. Sure, it's COVID, but there has to be more. Young women contracted COVID at high rates,¹ but not that high.
What the hell?
¹The mortality rate for young people was very low, but the case rate was upwards of 25-30%.
Health care deteriorated in all areas during COVID. People put off appointments if they could; nurses and doctors were more stressed out and (probably) made more mistakes; hospitals were understaffed.
Healthcare services have gone to hell across the South. Here in Mississippi, the largest hospital on the coast is stopping maternity services on April 1st & ER staff in rural hospitals are being trained to deliver babies (https://www.mpbonline.org/blogs/news/in-rural-mississippi-er-staff-are-being-trained-to-care-for-moms-and-deliver-babies/).
Exactly. This is a kind of mortality that we measure closely, and putting off care has disastrous effects.
A minor delay would have killed my mother twice over when she was trying for my sister.
And yet people put off health care in every advanced nation and yet none of them apparently had this increase in maternal mortality. So your explanation is easily disproved.
Serena Williams?
https://www.vox.com/identities/2018/1/11/16879984/serena-williams-childbirth-scare-black-women
That's a good point. You can't even be an international celebrity and get decent care, if you're female and black.
Someone who's business is knowing her health, even.
Having a major incision and blood thinners are contraindicated. One of her major problems was the massive hematoma in her abdomen caused by the blood thinner. So you can understand why doctors were reluctant to follow her initial demands.
I was a nurse for 40 years. I think the medical professionals initial response was pretty accurate. Health care workers won't just do what a patient says needs doing. Not for Serena, not for anyone. The obvious problem for her is that her nurse and MD had her medical history in their computers. That's the delay that was poor medical care.
Yes, but the ultrasound wasn't going to find any of the symptoms she indicated.
It would have shown a DVT (deep vein thrombosis) if it was present. DVT is a prime cause of pulmonary embolism.
In places in CA, they have set up "crash carts" in case there is trouble during child birth. In Atlanta (?), they have set up programs with more comprehensive care for the mother to be and new mothers. Both have helped. Not sure if they're being expanded.
The explosion of maternal mortality when Obamacare was being cut back--then the pandemic--is not unexpected. But the degree is still shocking. A few more states expanded Medicaid to fill the doughnut hole--that could help a bit in those places.
Access to hospitals has collapsed in poor areas. Malpractice insurance rates has made it almost impossible to be an OB-Gyn in some areas and even whole states. And now the abortion issue--maternal mortality will get worse for a bit.
Every unit in a hospital is supposed to have a crash cart. Even doctors' offices. But hey anything to save a buck, right?
In this case, a crash cart for problem pregnancies--not the typical having a heart attack crash cart. So extra fluids, blood products, what ever is needed to staunch bleeding, spikes in blood pressure, etc., with supplies on hand for the current patients. Almost like treating them as if they are going into surgery--just in case. Everything is lined up and ready to go so your not waiting on the blood bank, etc.
The blood bank is a big issue in most smaller (under 125 bed) hospitals. Most will have 4-6 units of emergency blood and no platelets or FFP. A cart can have central line kits but you dont need those often. It could have the emergency drugs you need for BP control but most OB floors already have those as will most EDs.
The general causes for the trends in an increase in mortality are, I think, understood and it is multifactorial. More heart disease, HTN, diabetes, obesity, lack of universal pre and post term care and older pts being some of them. Many OB units have closed but that means, usually, that pts will deliver in larger units with more experience. I honestly dont know if the potentially better care at a big place outweighs the delay in care. I know that some pts drive more than 1 1/2 hours to get to our OB unit.
I think we can only speculate about this spike until we see the causes broken down and look at where they are occurring.
Steve
Again, what you think of a crash cart is not what is a crash cart. Each unit has what it needs for resuscitation. Hell I've magnesium sulfate and tranexamic acid in my rig. OB/Gyn has mag and TXA but for different reasons. I've got five liters aboard but they get packed rbcs and plasma (refrigeration needs). I carry a 6 to 8 doses of narcan, they might have one. It's all tailored to the unit and what could happen. Mother/Baby has their bag of tricks, I've got mine.
COVID accounted for about 20-25 % of the deaths in 2021. Doesn't answer the bigger question but it was a huge problem. And thanks to the Trump administration and the Republican antivax agenda far too many pregnant women refused vaccination. And I am sure pregnancy loss, still birth and neonatal death during that time is through the roof as well.
So, the bottom line in this is the doctor's. That is where I would put my money. As a very old nurse, I have seen some Ob/Gyn's that I wouldn't send a stick to. They were more than frightening. The women were tough enough to have survived them and the nurses as their advocates. Yes, I'd say the doctors.
Did ob/gyns get that much worse between 2019 and 2021?
Re the general slow increase from 1990, one likely explanation is the rise in obesity; a study from France found, "The risk of maternal death increases with BMI; it multiplied by 1.6 in overweight women and more than tripled in pregnant women with severe obesity." https://www.nature.com/articles/s41366-020-00691-4#Abs1
Also, the denominator is live births; the birth rate has declined since 1990, and so it is entirely possible that the maternal death rate has trended upward because an increasing number of births are by mothers at higher risk .
As for the recent jump, while it might be true that "Young women contracted COVID at high rates, but not that high," note that the raw numbers in the cited CDC data are very low: "1,205 women died of maternal causes in the United States compared with 861 in 2020" (and 754 in 2019, per the data) -- out of more than 3.5 million births. I would think that it would not require all that many young women to contract COVID to cause an increase of 450 deaths out of 3.5+ million.
Some excellent comments here. Thanks to the thoughtful readership.
Whenever you see something like this especially with a big jump, the two obvious questions are
- what EXACTLY is being measured? and
- has the measurement changed.
For example is what's measured death while pregant, or death after pregnancy? The difference is huge: look at https://fullfact.org/health/deaths-following-childbirth/ which (for the UK) shows how large a factor suicide [and quasi-suicide, like drugs] is.
If it's deaths while pregnant, heart/blood/stroke type things seem to predominate, which suggests a place for the "increasing obesity as a slow increase" explanation, probably not helped by I'm assuming an increasing age of first birth.
The paper says that its definition is "the death of a woman while pregnant or within 42 days of termination of pregnancy, irrespective of the duration and the site of the pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes"
BUT
the "not from accidental or incidental causes" leaves a lot of wiggle room, especially if a policy decision was made at some point (in say 2017) that suicides and quasi-suicides, which had been considered incidental, were now to be considered related to pregnancy (perhaps in the hope of boosting mental health funds for postpartum depression or whatever). This strikes me as not unlikely. There's been a lot of work in the past five years or so on the hypothesis that postpartum depression is the result of dramatic hormone changes after the pregnancy, and that the worst effects can be alleviated by artificial hormones that give the body more of a tapered cutoff. This could have translated into how the data were defined and collected.
Suicide within 42 days of birth would never be considered incidental, but would always be connected to post partum depression,
As various explanations have been proposed, I would postulate that ALL of them have contributed to the rise. A perfect storm of negative influences.
* Medicaid and other medical access cutbacks.
* Covid (which doesn't have much to do with 2019) and vacc rates.
* Increasing obesity. Yeah, I'm "fat shaming." What of it?
* Doctors who should have retired, or stayed in retirement, but were hauled back on deck due to the Covid crisis.
* and, speaking of elderly doctors, increasingly elderly women getting pregnant.
As the great Al Gore remarked regarding global warming, "There is no silver bullet, just a lot of silver buckshot."
Yes.
Also a hypothesis that the payment system for OB-GYN is messed up - they get paid when the baby is delivered, all of the pre-natal care is "free." If the mother moves away, delivers in another hospital, etc then the OB-GYN doesn't get paid for the pre-natal care. In a time of general system disruption I can imagine the incentive to provide pre-natal care is even lower ... and then the burden of care becomes even greater in the stressed medical system. Probably not a huge effect overall, but one of the ways our system (doesn't) work.
And an alternate hypothesis to the old doctors ... maybe the experienced old docs decided now is the time to move on and we're seeing the consequences of younger, less experienced docs taking the load?
For the general slow rise, I would suggest an increase in the age of the mothers. Giving birth past 35 is considered "geriatric" and high risk.
@Jean__Fisch on Twitter has been digging into this spike in maternity deaths. They surged all across the South in 2021. It was coincident with a spike in COVID cases across the South, but Fisch admits he can't prove they're correlated.
https://twitter.com/Jean__Fisch/status/1635998717806276610?s=20
I ASSUME that Covid, both fear and actual illness, were major drivers of this change.
My wife is an ER Doctor. During peak Covid, lots of folks skipped important medical care, out of fear from the virus. Unfortunately, we may be seeing the results....
I have no solid theory why Covid fear might impact one racial group (black woman) differently than the broader populous.
We all skipped appointments not only from fear of Covid but also because our existing appointments were cancelled -- indefinitely. And good luck in getting a new appointment, back in those days.
"It's not because nobody cares about this."
That is true. Some people do care. Instead, it's because fewer and fewer people care about people that need care, even though it is ultimately the only thing that ever really matters.
Yes, the over-all rate of mortality from COVID for young people is low, but mortality for young people with COVID who happen to be pregnant is much higher. I couldn't find any comprehensive findings in a quick search, but according to "Maternal Mortality Jumped During COVID-19 Pandemic" at the University of Maryland School of Public Health site:
"COVID-19 was listed as a secondary cause of death in 14.9% of maternal deaths in the last nine months of 2020, with it being a contributing factor for 32% of Hispanic, 12.9% of Black and 7% of non-Hispanic white women giving birth."
COVID causes numerous health issues that could lead to death even if neither pregnancy nor COVID would end in death by itself. I wouldn't be so quick to write off COVID as a direct cause of maternal deaths after 2019.
But why the spike in the US and not in other nations?
Some of the issues mentioned in comments are also happening in other rich countries: increasing obesity, older mothers, covid infections, etc. Places like the UK have sizeable black populations and similar issues with obesity, maternal age, etc.
Yes, no one is saying it's just one thing.
I wonder how much poverty plays into this, as African American have approx 19.5% of their population living in poverty while for whites it's 5.4%. This may speak to the discrepancies between the groups, but maybe not the spike.
Possible Covid's impact to low income households was an add on to the trend. I'm curious how the chart works when adjusting for poverty. Does the difference between the groups remain the same.
Did poverty rates change that much between 2019 and 2021? There are many possible factors that could explain why the American maternal mortality rate is higher than it is in other countries, or why the rate is higher for black mothers than for white mothers, but which do not help to explain why the American rate jumped so much in two years.
For sure, the poverty rate didn't dramatically change. Overall it's been dropping after a short uptick in 2019. So it's not the driver of the spike. Just wondered if the Covid issues (hospital access, vaccination, etc) was a multiplier effect for those living in poverty.
Re: Prenatal care
When my daughter was born 25 years ago, we picked an OB, and it was a flat-rate deal, paid up front. One price included all prenatal care, water birth (the path we wanted) to C-section (the path we ended up on). We didn't pay extra for the version (she was breech a month out), nor for the complicated labor and delivery (after the version, she turned posterior, and got stuck). It would have been on us if we had up and moved during those nine months.
Interesting and different from my experience and those relayed to me. Is this b/c you were paying out of pocket, or was this how your insurer did it? Perhaps I'm point a finger in the wrong direction ...
I'll add that pediatricians I know had to fight with OBs in a small regional hospital -- the OBs were very resistant to sending patients to the University hospital when complications arose, saddling the pediatricians with infants that couldn't be supported (no PICU) and required transfer to the University hospital. The pediatricians saw this as mostly a money issue with the OBs.
The mortality rate over the past 30 years probably has some correlation to the increase in obesity and if you look at the three top causes of death (stroke, heart attack and bleeding) thru are all major risks associated with obesity. The rates of obesity are substantially greater in black women, which could help explain the racial gap. Also, about a third of maternity related deaths happen within a year post partum
Data like these scream 'artifact'. It's been a while since I looked at these data, but the official definition of 'maternal death' has changed repeatedly in the last 20 years, generally in the direction of including deaths that are more distant from the central concept. I am not saying maternal mortality has not increased -- or that it has -- but that you REALLY need to look carefully at how deaths are ascertained and counted, in a very granular way, to be sure that methods are constant over time, before you start wondering about what the real-world causes may be of such observations.....Full disclosure: I am speaking as an experienced retired applied epidemiologist. I have published on maternal and child health issues, but not specifically on maternal mortality.