The GAO published a report today about maternal mortality during the COVID-19 pandemic, and the nickel version is pretty simple: it got even worse from an already high base. You can read the whole report here.
But you might be interested in taking a look at maternal mortality pre-COVID. Here's the growth rate from 2007-2019:¹
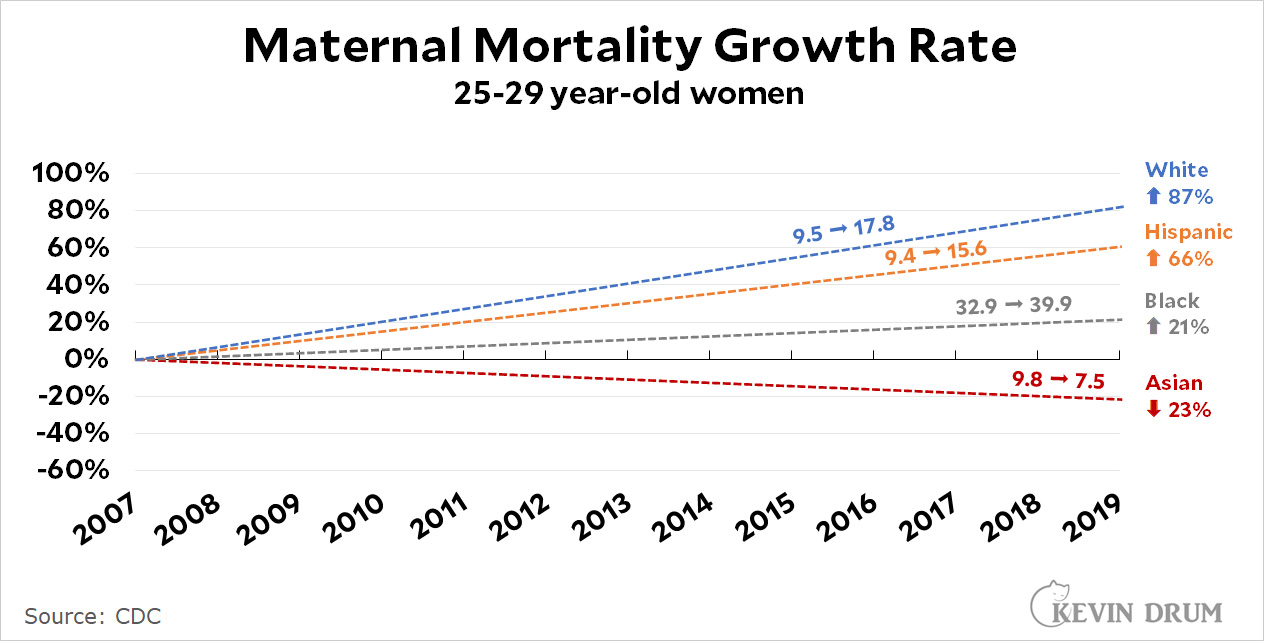 As you can see, the Black MMR has always been far higher than the others. However, white, Asian, and Hispanic MMRs started out about the same in 2007: high but not outrageously so. Since then the white and Hispanic MMRs have skyrocketed, while the Asian MMR has gone down a bit.²
As you can see, the Black MMR has always been far higher than the others. However, white, Asian, and Hispanic MMRs started out about the same in 2007: high but not outrageously so. Since then the white and Hispanic MMRs have skyrocketed, while the Asian MMR has gone down a bit.²
It's astonishing that we still don't have any good ideas about why our MMR is so much higher than the rest of the developed world, nor why it's increasing so much. Racism may play a role in the high Black MMR, but if so, why is the Hispanic rate lower than the white rate? It might also be due to a change in methodology for reporting MMR, but no one seems to think that's the culprit. Other explanations seem to fall flat too.
Based on this data, however, I might try investigating the Asian community to see what they've been doing differently over the past decade or two. They have cesarean sections at about the same rate as everyone else, so it's not that. On average, they have higher incomes and considerably more education than white people, which probably explains part of it. But what else? There must be something.
¹Why 2007-2019? For some reason the CDC WONDER natality database only goes back to 2007, so that's where I started. I ended at 2019 because there was a big spike in 2020. Since the spike was obviously COVID-related, it would have been misleading to include it.
²The Asian MMR is quite volatile because the numbers are so tiny: in a typical year there are only five or six maternal deaths, so a change of just one or two can make the MMR shoot up or down. However, the trendline is steadily downward.
My theory is diet, but I have no data to back it up. However I would love to see data that refutes it.
I was going to suggest this as the culprit as well, so I'll reply instead.
Increasing maternal size = gestational diabetes, eclampsia (hypertension and strokes)?
I’m sure they’ve looked into that, so probably doesn’t explain it well enough.
Is it that the white people having the most children are increasingly the lowest income and the biggest MAGA-heads, exactly those people least capable of providing a safe and nurturing environment, the and most likely to hate and resent the presence and responsibility of having a child in their lives?
'. . .and the. . .
Is the maternal mortal rate computed on a pregnancy by pregnancy basis or on an overall maternal deaths vs population basis?
Have you looked at the state by state distribution:
https://www.cdc.gov/nchs/data/hestat/maternal-mortality/2020/maternal-mortality-rates-2020.htm
(select per 100,000 births)
It may be necessary to look at geographical distribution at lower level than states, maybe even at individual hospitals.
Asians are diproportionately likely to live in California, which made a big effort to cut maternal mortality and succeeded brilliantly. My best guess is that high MMR is driven by our profit-driven healthcare system neglecting obstetrics and not making it a priority. Delivering babies is less profitable than a lot of other specialties, so it gets neglected. Doctors who do a bad job are tolerated. What we need is for someone to take the California model national. Make it a priority and hold hospitals accountable.
Like +25!
I still remember the pre-Obamacare days (Thanks, Barack!!) when if a woman wanted to buy a medical insurance policy, she had to pay a significant rider for pregnancy.
this
Women in the USA have gained a LOT of weight in the last few decades. That alone might explain a lot of it, but the addition of the really lousy health care system for the poor and vulnerable that we have only makes it worse. Poor women in the US tend more toward obesity and they tend to lack access to health care.
Yes, obesity is an obvious thing to look at. Weight data should be available.
Please stop with the we don't know lies. We have the data going back to 1800s Germany. We have journal articles from tracking rates from 1920 onward. Over and over again low-risk women working with OBs instead of Midwives increases infant and maternal mortality and morbidity.
Henci Goer has written books where 1/3 of the book is reprints of the studies she used.
Our OBs are not trained well but the US puts financial and legal pressure on more care not better care.
The causes are multifactorial but not mysteries. Most Pre-eclampsia is nutritional - the remaining being undiagnosed congenital kidney issues. We have know this since 1920 at least, but ACOG refuses to recognize this. Obstetricians are trained in and perpetuate bad care from not discussing diet, to recommending bed rest even when there is no data for it and significant data showing it is harmful. They have created a, " heads I win, tails you lose" scenario - where if you follow their advice and have problems the thinking goes, "Oh thank goodness for the doctor intervening, if he hadn't my baby and I could have died." There is never a question that the doctor's advice and intervention put mom and baby at risk unnecessarily in the first place.
Harvard Medical School started warning about trans fats and that eating cholesterol had no significant effect on cholesterol levels in the 1970s. Because of things like the standard of care and government subsidies where Congress set nutritional guidelines it took until about 2009 for any significant progress to be made.
Please before saying another word about maternal and infant mortality and morbidity take time to look at evidence based medical sites for maternity care like Henci Goer's or Australia's The Thinking Midwife. Even Midwifery Today can be a great resource.
Rising maternal age may play a role. The Great Recession caused a lot of middle class women to put off having babies for a few years.
The chart says the statistics are just for women aged 25 to 29.
One aspect to consider is age. MMR goes up significantly with age, and is about 5 times higher for women 40 and older than age 25-40. (Of course, there is no sudden jump at age 40, but the number starts going up significantly in the late 30s.) The US has seen a gradual increase in the age of mothers at birth that could explain some of the trend.
Of course, a number of complicating factors. Other countries have also seen age increases. Asian American mothers are slightly older than other groups but do better -- note though that age 30 versus 26 makes almost no difference, but 40 versus 36 does, so it depends on the precise shape of the age distribution. Black mothers are on average younger but do worse. Also, differences between states. California is just impressive, and its rate if half that of the second-best state.
I guess my point is, all other things being stable, an increase in age would give you a significant increase in overall mortality over the last few years. But age does not explain all or even most of the differences between different groups and states.
Look like the statistics just include mothers aged 25 to 29.
It's astonishing that we still don't have any good ideas about why our MMR is so much higher than the rest of the developed world, nor why it's increasing so much.
It's really simple.
Many people would rather eat sh*t than give a nickel to a negro, so they have de-funded healthcare, education and any public service that would help them especially if it could help African-Americans.
Most social issue that looks worse in the US than in other peer country can usually be put down to racism.
The above chart points to more than racism, as the dominate ethnic group (whites) have seen a much faster increase than all others. As he mentioned it isn't that racism doesn't play a roll, but it falls short of explaining the divergence in their rates of increase.
When you defund the healthcare system, sooner or later it's going to effect you, especially if you are poorer.
Maternal Mortality Rate by State 2022
Louisiana - 58.1 per 100k (Red State)
Georgia - 48.4 per 100k (Red State)
Indiana - 43.6 per 100k (Red State)
New Jersey - 38.1 per 100k
Arkansas - 37.5 per 100k (Red State)
Alabama - 36.4 per 100k (Red State)
Missouri - 34.6 per 100k (Red State)
Texas - 34.5 per 100k (Red State)
South Carolina - 27.9 per 100k (Red State)
Arizona - 27.3 per 100k (Red State)
It's clearly more than one cause.
I would guess Asians and Hispanics have a much better family support system.
As for whites, the dramatic increase could be in part the OB deserts in rural America.
And I agree diet may play a role, however they know that education and socio-economic status don't make a difference. If you think that talking with women about diet makes them change their habits, I will give you a moment to rethink that.
Can't wait to see what the MMR does in the red states that have outlawed abortion.
late comment from my mother in law house in a working class suburb in Montpellier France. Been there 4 weeks and i still have seen the so common overweight profiles we have in the US. Study show that French people have gain weight but they are still a few decades away from US.
Regarding MMR, this is all about socialism/communism (joking). There are mandatory (free) visits all along the pregnancy allowing to catch up risks early. For the lazy, no visits/ no Child credits payments.
Maybe relevant, maybe not, but black mothers use illegal drugs while pregnant at twice the rate of whites (and hispanic are lower than whites).
And before you want to chant rah rah whitey, the numbers for tobacco use among white mothers (I assume mostly lower class) are substantially higher than black mothers.
https://www.samhsa.gov/data/sites/default/files/Spot062PregnantRaceEthnicity2012/Spot062PregnantRaceEthnicity2012.pdf
As is so often the case in the US, segmenting by skin color rather than by *sub-culture* seems like an especially dumb way to collect and segment the data...
Part of the problem with your thesis is, when they control for everything they can control for, weight, age, income, education, drug use, etc, Black MMR is still usually double that of whites.
I would posit the difference in drug use between white and Black pregnant people is that Blacks are tested at twice the rate as whites, because, you know, racism.
Capitalism worked fine during the pandemic, thanks very much.
I think it's a matter of choice. If you look at a state by state breakdown, it lines up pretty well with politics. Blue states tend to do better than red states. There are exceptions like New Jersey and New York doing poorly and Utah doing well, but a lot of it is just political choice. New Jersey, for example, just passed some legislation to try and improve maternal health, so we may see some changes there.
The US used to be a can-do nation. If we had a problem, we'd fix it without the stupid arguments about ideology that seemed to hamstring Europe. Now, we're the inshallah nation, helpless and inert: it is what it is.
There appears to be no doubt that obesity increases maternal mortality:
https://www.nature.com/articles/s41366-020-00691-4
although the magnitude of the effect is variable in different studies. Anyone really interested in the racial differences and the increase should consider this quantitatively.
Which state has the relatively largest Asian population? Which state has done the best job of decreasing MMR?
~30% of asians live in California, and California is 17% asian (behind Hawaii at 54%).
https://missouriindependent.com/2022/07/06/states-with-strong-antiabortion-laws-have-high-maternal-and-infant-mortality-rates/
"California has the lowest recorded maternal mortality rate (4.0 mother deaths per 100,000 births). It’s not an accident, as this death rate plunged by more than 50% since the state passed the California Maternal Quality Care Collaborative in 2006."