
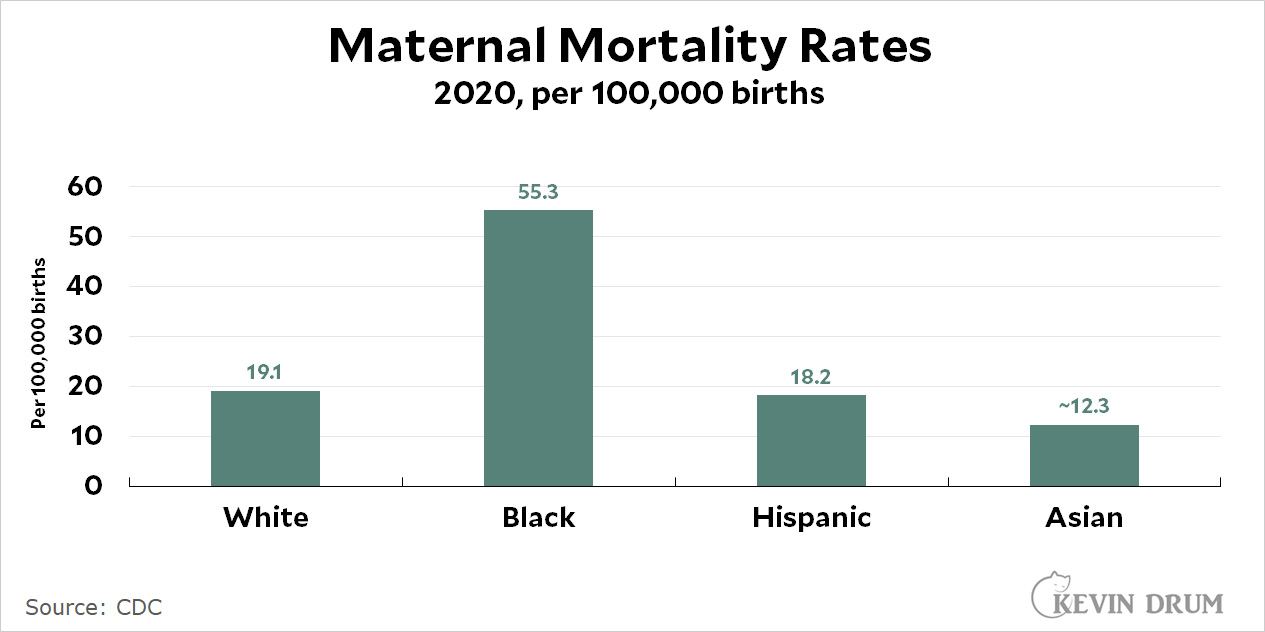
In the New York Times today, Jessica Grose interviews Linda Villarosa about the maternal mortality rate. It's worth a read, but first I'd like to reacquaint you with the basic statistics. First, here are the latest US maternal mortality rates by race:
 And here's the US maternal mortality rate over time:
And here's the US maternal mortality rate over time:
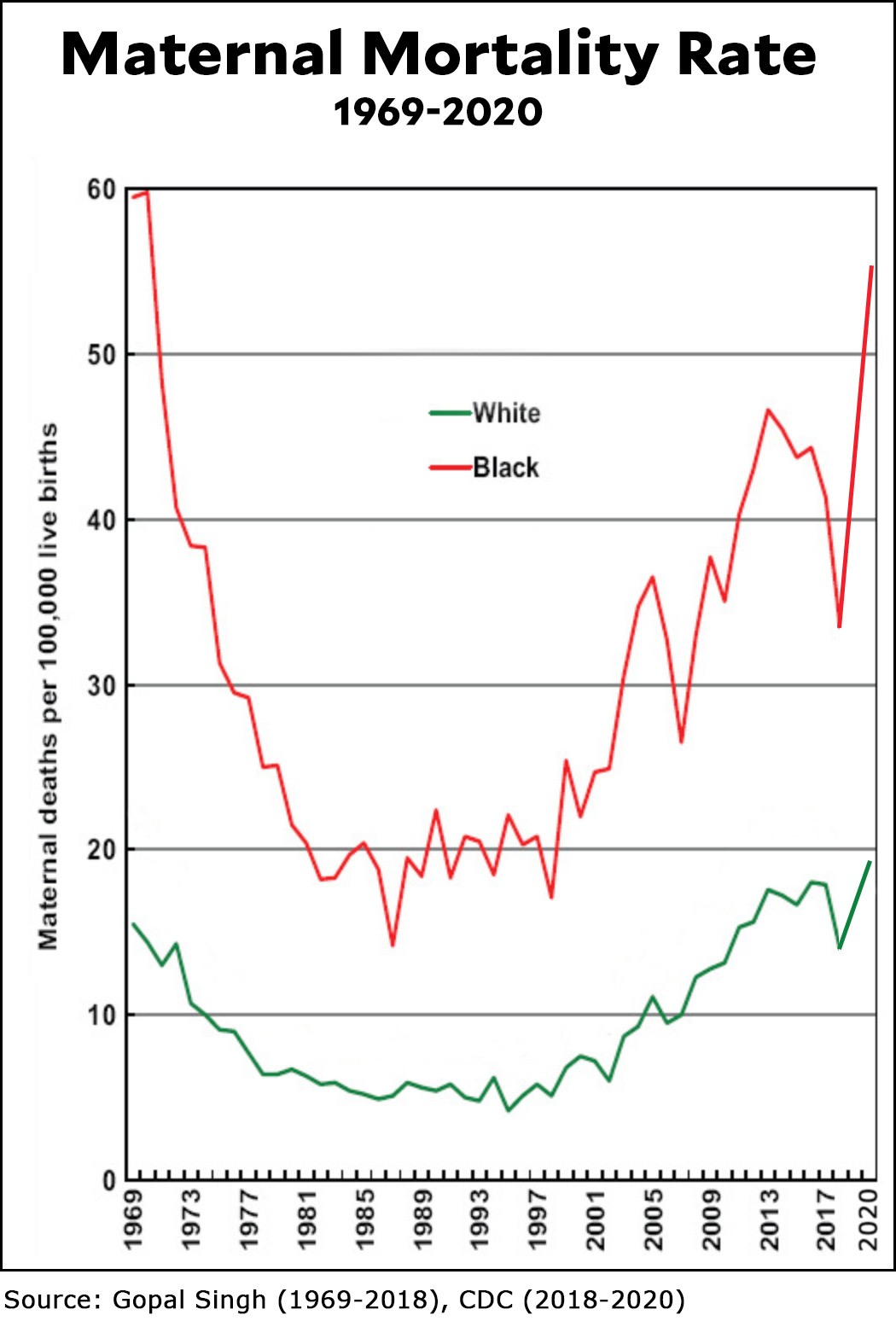 Everything here is nuts. The Black maternal mortality rate is nearly 3x higher than the white rate. And the maternal mortality rate for everyone has nearly tripled since the late '90s. Meanwhile, in Europe, the maternal mortality rate has been steadily dropping and is now about one-third the US rate.
Everything here is nuts. The Black maternal mortality rate is nearly 3x higher than the white rate. And the maternal mortality rate for everyone has nearly tripled since the late '90s. Meanwhile, in Europe, the maternal mortality rate has been steadily dropping and is now about one-third the US rate.
The big kicker is this: No one knows anything. No one knows why the rate has been skyrocketing. No one knows why the Black rate is so much higher than the white rate—while the Hispanic rate is a bit lower. In fact, we don't even have good data for the period from 2005-2018, so you'll see lots of different estimates for those years. (However, the big spike over the past three years comes direct from the CDC, which finally released new data a couple of years ago. It was the first in over a decade.)
And we're still in the dark about why Black women suffer such an astonishingly high rate of maternal mortality. As I said three years ago:
Poverty, education level, drinking, smoking, and genetic causes don’t seem to explain the black-white difference in maternal mortality. The timing of prenatal care doesn’t explain it. Medically, the cause of the difference appears to be related to the circulatory system, which is sensitive to stress. This makes the toxic stress hypothesis intuitively appealing, but it has little rigorous evidence supporting it. There’s some modest evidence that wider use of doulas could reduce both infant and maternal mortality, but no evidence that it would reduce the black-white gap.
Low income is weakly associated with higher maternal mortality rates, but it explains very little. The allostatic stress theory is appealing but probably wrong. And racism doesn't seem to play much of a role either.
It's the damnedest thing. The US rate of maternal mortality is crazy in multiple ways, and no one can produce a credible explanation. Every avenue of study turns up almost totally empty. I've rarely seen anything like it.
Well consider this, a paper found that oximeters used on covid patients regularly over-stated the oxygenation for blacks and hispanics. Consequently interventions started later based on these eroneous ratings, leading to higher mortality rates.
None of this was racism. But racial differences had real biological consequences. Something like that may be happening here. That is, the data for maternity are calibrated to white people but blacks are genetically different enough that they might require a different standards of care.
Is there a racial skew in Europe?
What the devil happened after 1997-98? That's a glaring inflection point. And whatever it was looks like it happened exponentially to black women too.
The end of medicare as we know it?
Compassionate conservatism?
Serena Williams story says a lot:
https://www.vox.com/identities/2018/1/11/16879984/serena-williams-childbirth-scare-black-women
Your answer is half-#idpol, so even with the other half being a dig on Bill Climpton for privatizing (if not outright ending) the safety net, in this Green Point, Brooklyn, listening bar you are at best half-correct.
so much better than usual 😉
NAFTA being more fully implemented?
Y2K?
Bill Gates...
The full effects of the end of leader gasoline in the US? …
The case definition of a maternal death, and the methods used to find deaths meeting the case definition, have steadily expanded over the last 20 years. That may not explain the whole increase, but it is a large part of what is going on. Either we used to miss a lot of true maternal deaths, or currently we are counting a lot of deaths that really wouldn't fit an a priori understanding of a maternal death, or both. For example, "Since 2003, states have been incrementally adding check-boxes related to pregnancy on death certificates to indicate whether a woman had been pregnant within the last year. As of 2018, all 50 states (and DC) utilize pregnancy checkboxes." -- https://www.mmhla.org/the-pregnancy-checkbox/#. The box is intended to flag deaths that might meet the CDC definition of a maternal death, which is currently defined as "a death while pregnant or within 42 days of the end of pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes." ..... This definition is a lot broader than those in use 20 years ago, and the detection methods are more sensitive.
My fellow data nerds may enjoy this methodologic piece. Among other things, it shows that the maternal mortality rate as reported using newest methods for 2018 is about twice what it would be if pre-2003 methods had been applied to the 2018 death certificate data.
Before you interpret health data trends over time, you have to understand how detection and reporting methods have changed over the same time.
I have seen nothing that suggests that these methods issues would artifactually increase estimate maternal mortality for black women and not for white women.
Richard Hopkins
https://stacks.cdc.gov/view/cdc/84769.
Maternal mortality also varies widely by state.
https://worldpopulationreview.com/state-rankings/maternal-mortality-rate-by-state
At 4 per 100 000, California is on the lower end of Western European rates and Massachusetts's is higher, but still only about the same as France, so it's not an inherently American problem.
Well there is another point.
It seems then a first conclusion is that a national level average among large ethno-racial groups is not going to be very useful for insights as too many confounding variables and too little internal coherency.
Sub-national (state) and break-down within the not-internally coherent ethno-racial groups at least by internal socio-economic status is likely to be needed to have any coherent insights.
Wow... Louisiana's rate is 14.5 times California's rate. I think the answer means digging into what's happening at a state level. It's interesting that of the worst ten states, nearly all are red.
Why are you surprised?
Pick any social index at random (health, crime, education, life expectancy, income, wealth) at least eight of the ten best states will be Blue and at least eight of the ten worst states will be Red.
Voting has consequences, if you vote for the Red team, you will get Red policy. Red policies are really bad for people unless they are very wealthy.
I expected a substantial disparity, but 14.5x? Few social indicators are that disparate between states.
Obesity -> preeclampsia
-> gestational diabetes
-> cerebral, cardiovascular events
Uninformed guess. I should read the NYT article before I speculate, maybe it controls for BMI.
I don’t know - doesn’t seem like a great answer. Did late 90’s coincide with an acceleration of obesity, more in AA than whites (but in both)?
After reading the NYT article, I think that, contra our gracious host Mr Drum, that racism could very easily play a significant role in the disparity. I also need think the medical system can be pretty sexist against women, treat them differently. (To the extent the genders are different tho, and if that makes sexism normal and not nefarious sometimes, idk).
I don’t find the Serena Williams story dispositive however. I’ve seen it before, and health care people missing something, acting like a patient doesn’t know what they are talking about, happens about 1000 times a day.
Because most patients really don't know what they are talking about.
If they did, we wouldn’t need medical schools. It’s the medical professional’s job to gather information in order to figure out what’s actually the matter. Some of that information comes from listening to the patient, and then using one’s professional knowledge to evaluate complaints, frame probing questions, and further evaluate patient answers. There is data on the value of well-conducted patient interviews.
Patients always know what they're talking about when they're simply describing their own symptoms. When they stray into opinions about diagnosis, then they don't know what they're talking about. That's why you consult with a doctor; so he can tell you what your symptoms mean.
I do think racial bias has a huge effect in two ways.
One is in the long term systemic bias when it comes to diagnosis and treatments (similar to what Special Newb said above), where a lot of medical standards or guidelines include racial considerations that were largely borne out of racism many decades ago, but still remain being used today. Here is a good article highlighting some of these:
https://www.newscientist.com/article/mg25233602-900-medicine-must-stop-using-race-and-ethnicity-to-interpret-test-results/
The second is the more nefarious racial bias of medical staff were people of color are simply treated less well than a white patient, which can be manifested in medical staff being more dismissive of the patient's complaints and symptoms for patients who are black. There's a ton of evidence over the years showing this happening very frequently at all levels of care (ER, hospitalization, family doctors, etc.)
There is evidence of sexism in medicine (it's obviously not severe; women continue to have higher life expectancies than men) but there is definitely no sexism in the treatment of pregnancy.
However, there are four racial groups identified. Hispanics and non-Hispanic whites have almost the same maternal mortality rate, although if there is racism I would expect it to affect Hispanics almost as much as Black people. The one that jumps out and is unexpected to me is that the Asian maternal mortality rate is only two-thirds of the white rate. I don't expect that is explained by white people receiving relatively inferior medical care.
Perhaps a state by state or urban/rural breakdown would be helpful. Another poster has noted that California has a much lower rate than the national average and I have the impression that there are a disproportionately large number of Asians in California. If I'm right, the Asians may have a lower rate because so many of them live in California (and perhaps in other low mortality states) or California may have a lower rate because so many Asians live there.
Serious research is called for.
This is a data area where a very strong first-order hypothesis should be that the broad ethno-racial categories 'black'; 'hispanic' etc are not really analytically useful, covering up huge amounts of phenotype variation (hispanic, e.g. covering everything from persons essentially European-Iberian descent through to mostly African or mostly Amerind descent; black equally covering persons of hugely varying biological descent) as well as internally huge amounts of socio-economic variation. Leading to group averages that are unlikely to be very coherent for major lessons.
Drunkposting again, I see.
Part of the problem is once again opioids.
https://news.vumc.org/2022/06/09/filling-multiple-opioid-prescriptions-after-childbirth-is-associated-with-a-50-increase-in-the-risk-of-maternal-death/
Is there any way to determine if access to birth control/abortion services plays a role? If it is harder to end an unwanted/difficult pregnancy, there may be a greater likelihood that there will be a death down the line.
✔✔✔
Perhaps the US has shitty prenatal care? i.e you have to have this baby, but we will not help you before or after birth. See Texas and the rest of the South.
There's one theory that American Blacks have circulatory and blood pressure problems because of the Middle Passage. Being kept below decks in chains en route to the US meant that a lot of people died. The survivors were those whose circulatory systems could endure the Middle Passage. The death rate is usually estimated at 15% which is pretty high, and slave living conditions further winnowed the gene pool.
This doesn't explain why white Americans do so poorly. Maybe it's our wonderful free market health care system.
Is per-live-births the best/only normalization? When used is there any accounting for births per woman? Is it indeed an independent roll of the proverbial die with each pregnancy? Normalization to per 100,000 women who give birth might be interesting.
The UN set up a number of targets prior to the new millennium
Target 5a was reducing by three quarters, between 1990 and 2015, the maternal mortality ratio and target 5b was by 2015 universal access to reproductive healthcare
Between 2000 and 2015 the number of women dying in childbirth in the world each year decreased from 543,000 to 287,000, a huge amount of progress.
Maternal survival has significantly improved since the adoption of these targets .The maternal mortality ratio dropped by 45 per cent worldwide between 1990 and 2013, from 380 maternal deaths per 100,000 live births to 210. Many developing regions have made steady progress in improving maternal health, including the regions with the highest maternal mortality ratios. For example, in sub-Saharan Africa it fell by 49 per cent.
… as you can see is the US of A the exception (together with a couple of war zones and countries plagued by other disasters)
The top countries are having something in between 3-4 deaths/100 000
Cannot this be correlated to the actions of the pro-life mob ?
They have succeeded in closing down a number of Planned Parenthood clinics and thus derived a lot of women the only affordable alternative they had for state of the art women’s healthcare
Your Swedish friend is just asking…
The story over at the Times starts off telling us that the maternal mortality rates have risen much more for black mothers than for whites, and that seems to be true when the CDC's figures for 2018 through 2020 are looked at, but it doesn't seem to have been the case in the 1995–2015 timespan, as studied by Gopal Singh at Health and Human Services. Is the CDC's methodology sound? Are we all convinced that maternal death among black mothers increased by half in two years? And a good part of this jump happened in 2019, so the pandemic can't be the cause.
For explanations of the longer-term increase all around, I wonder about maternal age and marital status. Are more mothers these days very young (teens) or rather old (>35)) than the mothers of 25 years ago? Are more of them single?
The average mother is older now than in the past. Teen births are down, and births to women over 35 are up.
If I were an enterprising researcher looking for a possible explanation, I's look at Catholic hospitals. Catholic hospitals are notorious for mismanaging miscarriages and refusing to perform abortions that are necessary to save the life of the mother. The bishopric has gotten more aggressive in recent years about enforcing its anti-abortion rules on Catholic-affiliated hospitals. Without hard data it's impossible to lay the problem at their feet, but it's a plausible explanation and it should be looked at.
And increasingly in some rural areas the Catholic hospitals are the only ones left. UGH. Yes they are screwed up -- in a sane country they wouldn't be allowed to only offer substandard care.
In many European countries, the Catholic church used to run the hospitals. In every one but Ireland, the government eventually realized this was a bad idea and took them over.
The racial differences are obviously going to be cultural in all its pernicious multitudinous 'glory'.
The interesting/perplexing phenomenon is the matching trends overtime. Some good thoughts above. What about the ageing of the OB-GYN doctors? Late stage doctors often make more mistakes than mid career. Wonder if there are trends in number of practitioners going into OB-GYN over time?
I wonder if Kevin "get the lead out" Drum has considered something else?
Is it possible it's tied to the food supply here in the U.S.?
We use LOADS of fertilizer, pesticides and insecticides while growing our food and have had to since the baby boom. We also genetically modify some foods and store them in both climate and atmospheric controlled warehouses to make them last longer.
Are we looking at another lead in the water situation?
Japan is far far worse than America when it comes to food additives and their rate is the same as California's, 4/100k.
I suspect a connection to extreme obesity.
1. Maternal death is very rare in the US - even among black mothers it is only 1 out of 2,000. You need to be an outlier or very unlucky to die in childbirth.
2. The risk of maternal death goes up fast with obesity. See https://www.nature.com/articles/s41366-020-00691-4#:~:text=The%20risk%20of%20maternal%20death%20increases%20with%20BMI%3B%20it%20multiplied,obesity%20could%20improve%20their%20outcomes.
"The risk of maternal death increases with BMI; it multiplied by 1.6 in overweight women and more than tripled in pregnant women with severe obesity. Training clinicians in the specificities of care for pregnant women with obesity could improve their outcomes."
3. Extreme off the scale obesity is obviously going to be riskiest.
4. Rates of extreme obesity (BMI 40 and up) are highest among blacks, about equal among whites and hispanics, and least among Asians - very similar to the maternal mortality numbers. https://news.gallup.com/poll/155735/blacks-likely-obese-asians-least.aspx
5. Extreme obesity is also getting more common over time, also explaining the numbers.
Almost all these comments accept that the data as displayed are a correct reflection of reality. As I noted in an earlier comment, our methods in the US for detecting and counting maternal deaths have changed substantially over the past 20 years or so, and those changes account for at least part of the increase in reported rates over time. I think the black-white disparity is real, but I am quite dubious that the real time trend is correctly reflected in the time series displayed.
FWIW: although I am not specifically an expert in maternal mortality or how to count it, my professional interest and expertise as an epidemiologist is in public health surveillance methods. And that experience tells me emphatically, when you see a surprising trend, look for data artifact before you interpret it. Same when you see a trend that seems to confirm your pre-suppositions.
Richard Hopkins
My fellow data nerds may enjoy this methodologic piece. Among other things, it shows that the maternal mortality rate as reported using newest methods for 2018 is about twice what it would be if pre-2003 methods had been applied to the 2018 death certificate data.
Before you interpret health data trends over time, you have to understand how detection and reporting methods have changed over the same time.
I have seen nothing that suggests that these methods issues would artifactually increase estimate maternal mortality for black women and not for white women.
Richard Hopkins
https://stacks.cdc.gov/view/cdc/84769.
Racism plays a huge part in the m and m of black women. Likely for other races also. This is from a nurse who watched how the staff, doctors and nurses treated folks differently if they were black. It is disgusting but there it is....