This is a drone's eye view of the Port of Los Angeles (top) and the Port of Long Beach (bottom). Today marks the first meeting to discuss a new labor contract for dockworkers on the West Coast, about two-thirds of whom work at either the LA or Long Beach ports. Backlog at the two ports is currently down to 35 ships from a high of 109 back in January, but that could all fall apart if talks fail to conclude by July 1 and dockworkers go on strike.
October 9, 2021 — Wilmington, CaliforniaOctober 9, 2021 — Long Beach, California
I got an email yesterday from a regular reader who asked about something I had been mulling over too: If Roe v. Wade is overturned, can Indian tribes open abortion clinics of their own on tribal land? If they did, could they use them to attract patients from nearby states that have banned abortion?
In other words, the casino model but for abortion. Unfortunately, I had already taken a superficial look into this and every hyperlink I clicked just seemed to make the answer even more vague. Here's what I found out:
Legally, Indian tribes have the sovereign power to make their own decisions on abortion. This will probably end up in court eventually because everything ends up in court eventually, but as near as I can tell there's not much controversy about it.
In practice, health care on tribal land is provided by the Indian Health Service, a federal agency. However, the IHS is bound by the Hyde Amendment, which prohibits federal funding of abortion except in cases of rape, incest, or the health of the mother. In reality, though, IHS clinics and hospitals perform no abortions at all, and given the widespread poverty in Indian Country this means that most native women have no realistic access to abortion.
To address this, tribes could raise money to build their own abortion clinics, which would provide access to abortion for both their own people and for residents of nearby conservative states. .
(In 2006, the president of the Oglala Sioux Tribe, Cecelia Fire Thunder, tried to do exactly this. The tribal council had previously voted unanimously to ban abortion, and after a battle that remains infamous to this day, they impeached her. You will be unsurprised to learn that the council was mostly male. You can read about it here.)
Needless to say, a program of opening abortion clinics on tribal land depends on whether tribes want to attract outsiders to abortion clinics. This likely varies from tribe to tribe, just as it does from state to state. Some tribes are conservative about reproductive health and have already banned abortion in their own constitutions.
For what it's worth, there appear to be no Planned Parenthood clinics on tribal land anywhere. There are a few independent clinics here and there that provide abortion services, but their numbers are minuscule.
Of course, things are changing. Access to abortion may be limited in tribal areas that adjoin conservative states, but if these states ban abortion then tribal access to abortion will essentially be banned too. This is likely to change attitudes. It will also likely change the odds of attracting outside funding for abortion clinics.
This all adds up to a great big "I don't know." But perhaps there are some people who know more about native culture than me and can offer a few informed opinions in comments.
Let's test the economic mettle of my readers. Do you think inflation went up, down, or stayed the same last month? The BLS will report their results on Wednesday at 8:30 am Eastern time.
I mentioned in the previous post that (a) national polls about abortion are useless, and (b) attitudes toward abortion have been very stable. So here's a set of (a) three national polls (b) showing that attitudes toward abortion have become more liberal over the past couple of decades:
These three polls are all reliable and have been surveying abortion for a long time. Unfortunately, their question wording is just different enough that there isn't a single response that's common to all of them. So for GSS and Gallup I showed the share of people who think abortion should be legal in all cases, and for Pew I showed the number who think it should be legal in all or most cases.
The outlier here is GSS, which says that 54% of Americans think abortion should be legal in all cases. This is far different from other polls, which range in the 20-30% region for this question.
Also worth noting is that in polls that break down responses by political party, the reason for the liberalization of views is strictly due to Democrats. Republicans have stayed about the same for the entire time.
Just a quick note to anyone proposing some sort of compromise position on abortion because it polls well: Don't bother. National polls don't matter. The only thing that matters is how well your compromise fares in each state. If it's really popular in, say, Indiana, then maybe there's a chance of getting the Indiana legislature to pass an abortion bill that's more moderate than an outright ban. If it's not, then they won't.
By my rough count, there are maybe a dozen states where there's a chance of passing some kind of compromise. But keep in mind that this includes purplish states where the bad guys might persuade the legislature to make abortion regulations a little tighter. We're not the only ones pushing for whatever we can get, after all.
Anyway, that's it. For the time being, national polls and national support for various abortion proposals don't matter. That's a long-term PR job that neither side has been very good at.¹ Right now, all the fights are at the state level.
¹National attitudes on abortion have been famously stable for the past 50 years. Neither side has made much progress, although there are a few polls that show a bit of pro-choice movement over the past five years.
The nation's press has finally caught on to the nation's shortage of infant formula. That's good.
What's not so good is that they keep mindlessly repeating the same phrase over and over: "The out-of stock percentage has reached 40%." Or, even worse, "40% of baby formula was out of stock in more than 11,000 stores across the country."
What does this mean? That 40% of stores are out of stock? That store shelves have 60% of their usual quantities? That 40% of the time shelves are empty?
None of the above. "Out-of-stock percentage" comes from Datasembly, an industry analyst, and it's a term of art. Specifically, it refers to the percentage of SKUs that are unavailable.¹
SKU is short for stock keeping unit, and it's yet another term of art. Every single product a retailer sells is an individual SKU. A seven ounce Hershey bar is one SKU. A four ounce bar with almonds is a different SKU. A four ounce Cadbury fruit-nut bar is yet another.
In other words, an OOS percentage of 40% means that 40% of infant formula SKUs are out of stock these days. If you normally purchase Similac Advance in the 32-ounce size, you might find that you can't get it. But Similac 360 Total Care in the 8-ounce size might be easily available.
The good news for harried parents is that that one brand of formula is as good as another, nutritionally — so if their regular brand is out of stock, parents can use another brand as a substitute with no concerns.
“It’s okay to switch between brands if needed. They’re generally the same ingredients, but maybe tweaked in very small, minimal ways, but you can switch between brand names or off-brand names from the supermarkets and the bulk stores.” Tom Herrmann, a spokesperson for the Arizona Department of Health Services, told a local Arizona CBS affiliate.
The formula shortage really is bad news, and it's gotten worse since a major recall earlier this year. But if it's causing you problems, check with your doctor. Unless your infant has special requirements, you can probably just buy whatever's available if your favorite brand is out of stock.
¹If you want to sound effortlessly knowledgeable about this stuff, SKU is pronounced skew in normal conversation. Example: "We did an audit and there were 237 skews that were misidentified in the MRP database." ²
²MRP stands for Material Requirements Planning. It's pronounced Emm Are Pee, and it's the software used for forecasting, BOM management, ordering, and other factory floor operations. Example: "We use Oracle for MRP but we're thinking of doing a big switch to SAP." ³
³BOM stands for Bill of Materials, the list of all the bits and pieces that go into a finished product. Note that MRP can also stand for Manufacturing Resource Planning, which is typically referred to as MRP II. The biggest MRP packages these days go by the name of ERP, or Enterprise Resource Planning. These software suites basically run everything from MRP to financials to human resources and more. Two of the biggest suppliers of ERP software are Oracle and a German company called SAP.
I'm not sure what this is, but an image search suggests it might be a stonecrop of some sort. Maybe a white diamond stonecrop? For those of you who want to take a guess, it's about two feet across and was growing out of a vertical face (mostly just dirt, though, not stone).
After overturning abortion protections, is contraception next for the Supreme Court? A couple of years ago Gallup polled Americans about the moral acceptability of various issues and this is what they came up with:
A Pew poll taken a couple of years before this one came up with an even lower number: nationally, only 4% of the population opposed contraception on moral grounds.
I wish we had state-by-state polling for contraception, but given these national results I'll bet there's not a single state where more than 10% of the population opposes contraception in general. The number is certainly higher for emergency contraception, but oddly, I can't find any survey data about that.
There's no question that emergency contraception is controversial in the same states that oppose abortion, and this is something the Supreme Court will probably rule on eventually. But ordinary contraception? I doubt it's in any trouble. The Supreme Court might pretend that it doesn't care about public opinion, but they're not going to endanger access to something that's approved by 92% of the country. Even Sam Alito isn't that stupid.
Can someone tell me what's going on with the Russian army? Nothing I've read truly seems to explain its epic incompetence. I mean, I know all about the maintenance issues and the logistics and the pallets and all that stuff, but Russia's operational problems go way beyond that. They seem literally unable to accomplish anything.
The longer this goes on, the more boggled I am. Is US intelligence equally boggled?
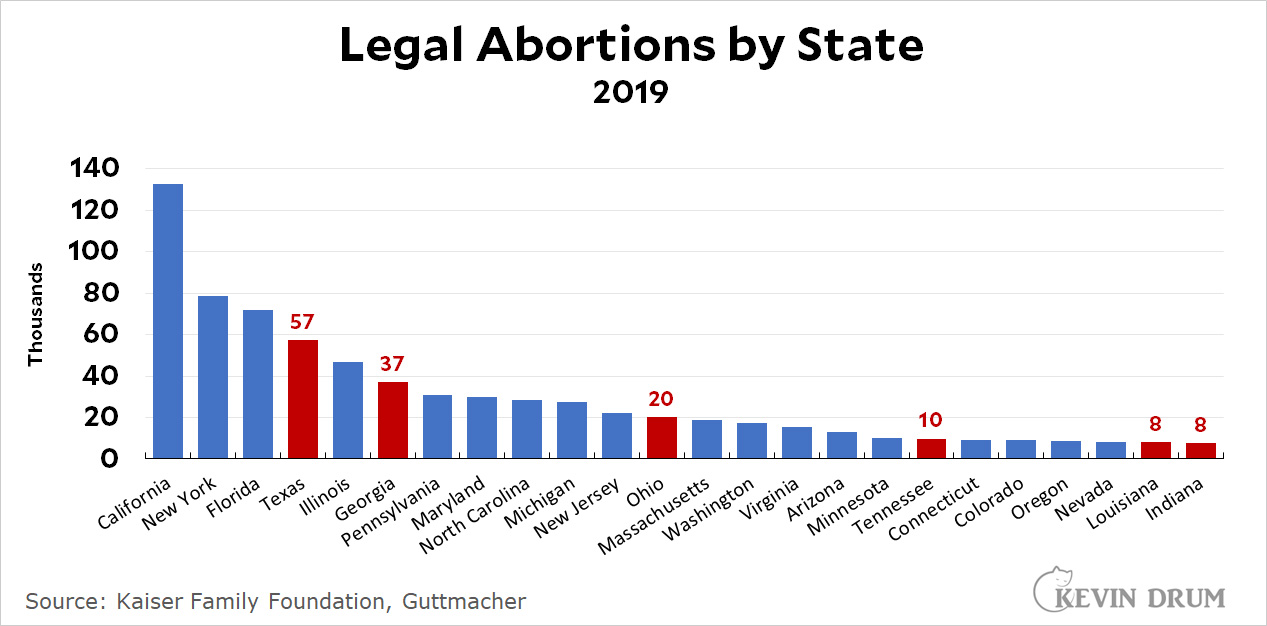
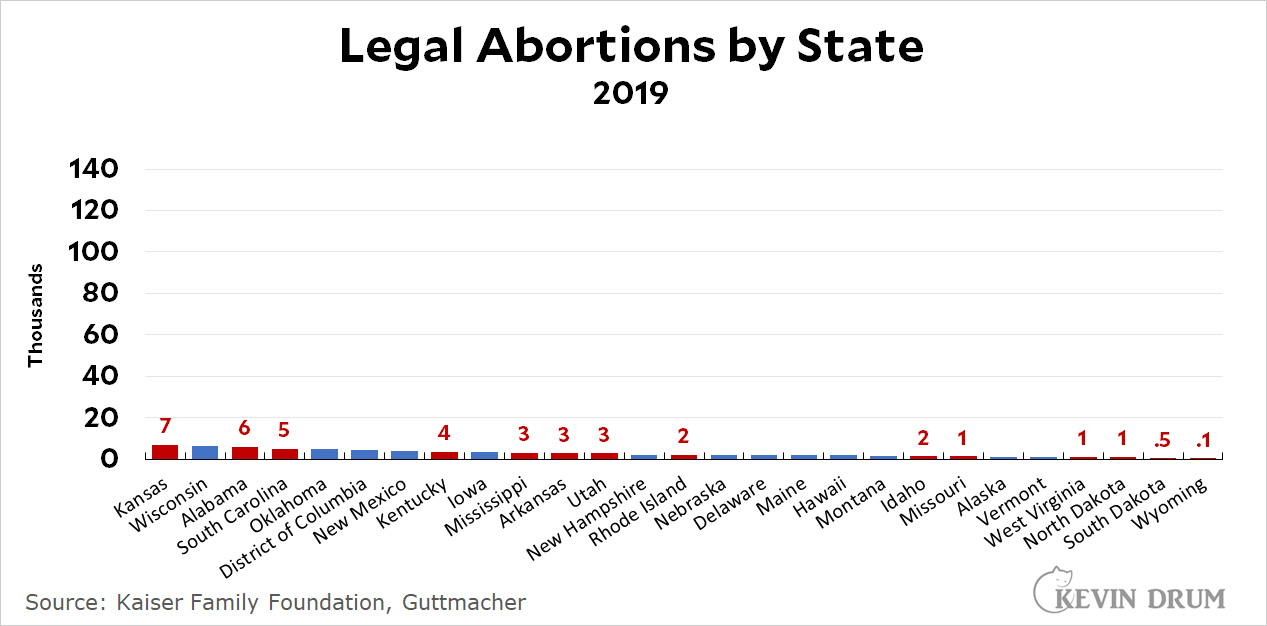
Here's a look at how many abortions are likely to be halted after Roe v. Wade is overturned and conservative red states have passed laws outlawing abortion (red bars):
I've counted any state with a 50% majority opposed to "all or most" abortions as a state likely to pass a law banning all or most abortions. As you might guess, most of these states have already passed laws making it difficult to get abortions, so they don't account for that many to begin with. They make up about 22% of the 800,000 abortions performed each year, with half of that in Texas and Georgia alone.
Obviously there are other states, like North Carolina and Florida, that might ban abortion as well, even though majorities don't support it. And there are some in the opposite category. Nevertheless, if we want to provide abortion services to everyone who's cut off from them by the Supreme Court, this gives us a rough baseline number: about 3,000 per week. Add in another couple thousand who have already been partly cut off, and then figure an average out-of-state abortion costs about $1,500, and we're talking something like $7-8 million per week.
If progressive organizations—and progressive billionaires—are serious about this, it's not really very much money at all.