
Here is something I'm curious about:
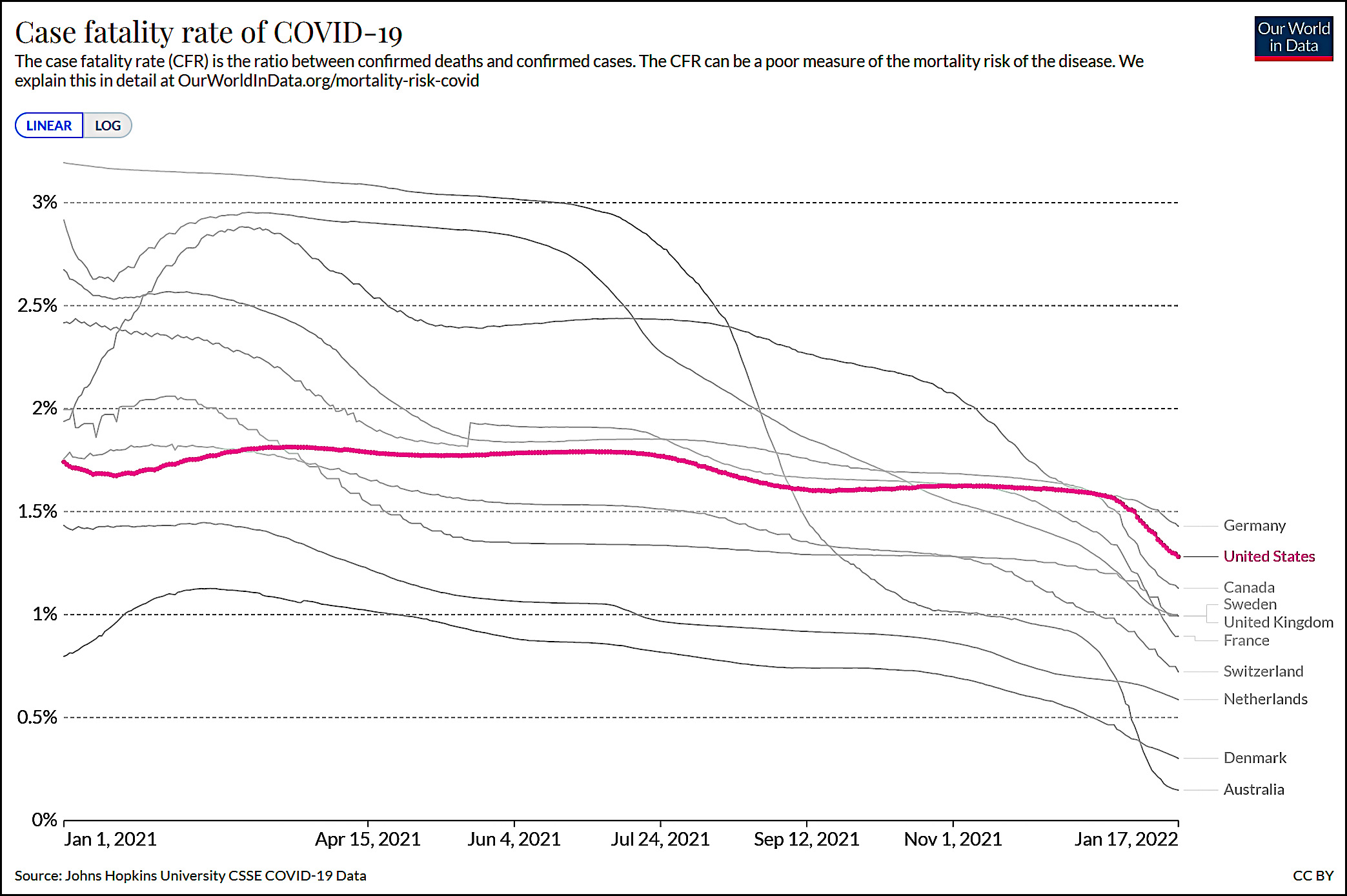 This chart shows the case fatality rate throughout all of 2021. CFR is a measure of the percentage of people who die after being infected with COVID-19.
This chart shows the case fatality rate throughout all of 2021. CFR is a measure of the percentage of people who die after being infected with COVID-19.
CFR is an imperfect measure, but it's still striking. At the beginning of 2021 we ranked #3 out of the ten countries I've charted. Today we rank #9, and we'd be dead last if not for a sudden burst of progress over the past four weeks.
What's going on here? Why have other countries all made considerable progress in cutting the number of COVID deaths while the US has been flat until very recently? It can't just be a result of vaccinations. We might not be as vaccinated as some countries, but we've gone from zero to 60+ percent over the past year. It's not as if we've done nothing.
So what's the answer?
Maybe the United States was testing a lot more of its people back in January 2021 than most of those other countries were, and by now that has changed.
Take a look here:
https://ourworldindata.org/grapher/daily-tests-per-thousand-people-smoothed-7-day?tab=chart&time=2021-01-13..latest&country=GBR~ITA~AUS~CAN~NLD~DEU~SWE~FRA~CHE~USA
Sorry the link here is chopped up, but if you copy the whole thing as text and use that as your URL, you might get the picture I was looking at.
Another try.
https://ourworldindata.org/grapher/daily-tests-per-thousand-people-smoothed-7-day?tab=chart&time=2021-01-13%2e%2elatest&country=GBR~ITA~AUS~CAN~NLD~DEU~SWE~FRA~CHE~USA
Nice. Thanks for the link.
CFR is more likely a measure of the percentage of people who die after having a confirmed positive test not who die after being infected. If you have poor testing then you have a higher CFR because you miss so many mild and asymptomatic cases.
That and I doubt it is unique to covid. I suspect for lots of medical things we have a higher percentage of poor outcomes due to things like obesity prevalence and unequal access to the healthcare system.
If you have poor testing then you have a higher CFR because you miss so many mild and asymptomatic cases.
Exactly. It seems likely at least some of the elevate CFR of the US is linked to failure to confirm as many cases as other countries (ie, lower testing capacity). Obviously people who are admitted to the hospital with covid symptoms will be tested/confirmed, so, these "confirmed cases after hospital admission" will account for a higher percentage of total confirmed cases in the US than elsewhere. And a certain percentage will results in deaths.
I expect vaccination lagging and higher comorbidities play a role, too.
I have two possibilities; cloustering of unvaccinated higher risk people like older, politically motivated anti vaccers or higher risk populations with poor healthcare access (e.g. Original Inhabitants) the other is lower rates of booster shot (US has the lowest rate of any of your chosen countries). A subset of the booster shot issue is that, due to a lack of a national health system the booster shots (and all the vaccination shots) may not be as well targeted to the highest need population.
There is a CDC study that shows non-covid mortality rates are much higher among the unvaxxed vs. vaxxed. This supports the idea that there is a risk selection effect for vaccination. People who choose to get vaccinated care more about their health than the unvaccinated and so have better health overall. So why especially in the US? Perhaps the variance here is greater due to accessibility of healthcare. At any rate, if this were true, it would inflate the apparent effectiveness of vaccines as shown by vaxxed/unvaxxed hospital admissions, ICU admissions, and death.
I'll take vaccination rates for $500. In January 21, we had the roughly the same vaccination rates as other countries (close to nothing). Now we (presumably) lag far behind, so more deaths. Just speculation, as I'm to lazy to look up anything to support this.
fyi:
https://ourworldindata.org/covid-vaccinations
Why does deaths fall as vaccinations increase but not cases?
Well, a, it does, but b, vaccination prepares the immune system to fight off the disease - and the fastest testing merely detects an immune response.
The vaccine isn't a mask or bubble that stops the virus from entering your body.
Obesity? The US has some of, if not the highest obesity rate in the world. In addition, Covid-19 kills by destroying the lungs ability in intake O2. Since obese need more oxygen than regular folks to keep themselves alive due to having more body tissue to support, it would make sense that they would die at higher rates.
Another thought might be that our healthcare system is more on cure than prevention, which means that there may be more older, obese people who are extremely susceptible to Covid's method of killing.
But this is just a thought, and a rather obvious one at that. Surely if mortality coincided with obesity to such a degree, some statistician somewhere would be shouting on the rooftops about it.
Come to think of it, is Peru's altitude related to its incredibly high covid mortality numbers? Less oxygen in the air already that high up...
While Peru does have a fair number of people living at altitude, so do Colombia, Ecuador, and Bolivia.
The majority of Peru's population lives along the coast (mostly in and around Lima). Here's a cartogram showing the population distribution: https://worldmapper.org/maps/gridded-population-per/
Of the cities listed, only Arequipa and Cusco are at high elevation; the others are coastal.
Okay. It was idle speculation anyway. What happened in Peru was a nightmare and one the world should study. If we can learn whatever factors contributed to such a perfect storm, we should mitigate them if at all possible. Something like .6% of the country up and died, which is over twice the death rate of most other western nations, including the US, Brazil, and most of Europe.
We are all fat and that has the biggest risk of death. Also our medical system has been repeatedly overwhelmed compared to real countries.
How do Mexico & the United Kingdom* stack up compared to US? They are 2 & 3 on overweight/obese indices.
*Who's the sceptic tank now, wankers?
There was a discussion a while ago that the US PCR protocol uses more cycles, so more amplification and detection at lower levels of virus. That means we could pick up more cases. I think other countries made more use of antigen type tests, also less sensitive than PCR tests.
Following trends in case numbers is useful to see where the outbreak is going--and long as you're also looking at positivity. But cases detected is a function of actual cases, amount and type of testing, positive test rate, and rules for testing eligibility. That's why you were plotting deaths, not detected cases. A better measure of outbreak's severity--but by definition, a lagging indicator.
Good points.
There was a discussion a while ago that the US PCR protocol uses more cycles, so more amplification and detection at lower levels of virus. That means we could pick up more cases.
That should result in lower, not higher, CFR in the United States, right?
Yeah, it would seem so. Maybe this difference in testing was more in evidence early on, when the United States' CFR was lower than most of the countries on Kevin's chart.
Vaccination rates (including boosters and the geographical clustering of unvaccinated people), testing rates, and high income inequality/lack of socialized medicine/social safety net are likely what's setting the US apart from its peers.
Folks deny Covid, don't vax, party on like there are lots of tomorrows, don't mask, join huge crowded events, eat out at crowded restaurants, on and on. Did you want more?
I am staying as far from these folks as possible.
School closures, on line learning, free proper masks and Covid vax sooner, rather than later are also issues. t-Rump was the one who really held things up. Biden and co. had to play catch up.
We also need 1(one) person to give us the news, restrictions, etc. on Covid rather than dualing politico's. Thank heavens for Fauci.
Delta hit certain places in the US like Florida and Texas very hard. If you go over to worldometers and compare the 7 day averages of those states vs California you will see what I mean. I would guess that the general attitude of invulnerability in those states had something to do with the high death rates there and that translated to more deaths in the US.
Not only did Delta hit them hard, but Omicron is hitting them hard now--just a few months later. 'So much for "natural immunity".
The problems with relying on post infection immunity is that it is dependent on the difference between the original version the patient got sick with and the new version they got exposed to. They have to be essentially similar in order for previous infection and vaccinations to work
We should be tweaking the vaccines for Omicron. We cannot "tweak" the bodily immune response UNLESS you get sick
The tragic mistake was NOT making a DELTA specific vaccine. We should NOT make the same mistake again. Tweak the vaccine.
They are tweaking the vaccine, but that takes years, or at least months, while a variant comes out in weeks.
"What are breakthrough infections?"
"Not as deadly"
Just a speculation, but could the pattern be partially due to the popularity and widespread use of ineffective remedies among the anti-vaxers in the US? Are these quack remedies as widespread in other counties where CFR performance has been improving steadily?
Why is the US death rate from COVID-19 so high?
Doctors per 1000 people, US vs EU,
https://i.redd.it/ha8nrtgko7981.png
It would be interesting to chart the CFR by states in the US. Plots for States could be grouped by covariates such as physicians per 1000 people, among many possible explanatory factors, political and otherwise. Is the poor performance accross-the-board, or are some states doing much better or worse?
Interesting how drs/1k correlates with population density...
It actually does not look that way.
C'mon Kevin
YOU'RE the one that tied lead in pipes to crime
So, think of it this way
Take the American diet that existed say from 1925 through the end of WWII.
Then check that very same American diet from 1955 to present
Make the correlation between diet and diminishing exercise.
We raised an ENTIRE generation (baby boomers) who believed that they DESERVED to be able to eat what they want, drink what they want, smoke what they want, while buying 1 2, or 3 cars for the family and DRIVING them everywhere (only to stop at those new fangled fast food places like Kemps, Jack in the box and some new place called McDonalds).
As American consumers grew in numbers, our exercise became less vigorous and our diets became laden with salt, fats, preservatives and other things that people in the 20s/30s. and 40s just didn't have.
NOW we are a nation - the MAJORITY of which have comorbidities such as obesity, diabetes, high blood pressure, Crohn's, IBS, and a host of other immuno compromising diseases
And you ask this type of stupid question
Do the study. THIS is why we toss variants around the population like Cheetos in the living room. We have too many people with impaired immune systems. We cannot rely on a CONSTANT and effective "natural" response to viruses because of all the things stated above.
We are exceptional alright.
Maybe a different way to look at the question is:
"why did the CFR not drop as vaccinations were deployed throughout the population?
First, what isn't the culprit: lack of masking/distancing: but these reduce cases, not CFR. Similarly, can't be too-low levels of vaccination, b/c again, that would reduce "confirmed cases" (the vaxxed have more asymptomatic or really mild cases, right?) We're left with:
1. comorbidities in the patient population
2. weakness in medical treatment system
Or at least, it would seem to me. Now why that would change in recent weeks, is .... a mystery. Neither of these seem like they'd change over a short period of time.
Omicron's decreased lethality. If it was as lethal as, say, delta, we'd be seeing 10k deaths a day right now. Note that CFR is dropping for all countries, not just the US. Sadly, the sheer number of cases will still drive a large number of deaths, but fortunately, not what Delta would have done.
Omicron is essentially the end of the pandemic in the beginning of endemic covid. We will never be rid of it now. It is almost as contagious as the measles.
Masking does decrease the CFR - because the dose of the virus does matter in the immune response.
Yes.
This point is simply not emphasized enough. Viral load seems to be a big factor in the eventual result of an infection.
If omicron is contagious enough that we have to accept that likely we all will eventually get it, makes sense to give up on the idea that anything like masking, social distancing , or vaccines will prevent that infection .
But we can still influence the result by viral load . And things like masks can help there. Perhaps even a decent strategy to deliberately NOT mask in situations where the viral load , if you catch it, will likely be low. Such as shopping where you will only have brief pass by contact with any specific contact. But mask when viral load would be high, like at a gathering with a number of people in close contact for a sustained period. So as to perhaps decrease the chance of a high viral load infection while increasing chance of a low viral load infection.
But I think many reverse this and end up masking in situations with multiple brief contacts with strangers but unmask when with friend or office workers they know for a long time.
Because almost every time I read a story on CNN about a “perfectly healthy” person dying of covid, it is accompanied by a photo showing someone at least 30lbs overweight.
My guess would be our fragmented, understaffed, inefficient health care system. It's lagged behind the rest of the developed world for years, and COVID has sent it into meltdown.
Lots of folks in here blaming obesity, and I recommend they read this post and see if they can refute it: https://www.lawyersgunsmoneyblog.com/2021/09/covid-and-the-moral-panic-over-obesity
The research cited by lawyersgunsmoney actually shows convincing evidence of a harmful effect of obesity - the greater the obesity the greater the danger of covid. But as that and other actual research has shown, the current BMI is not a good guide to health. Being "overweight" should probably start at well over the current 25 value.
BMI is not necessarily a good ,measure since it measures eight and weight, nor body fat percentages.
According to the CDC, a BMI of 30-35 is associated with a longer life span than a lower one, but that's in older people. I have no idea of why this hasn't filtered into the BMI guidelines.
Why?
- We have a fee-for-service healthcare system that discourages the marginally insured and uninsured to avoid early intervention.
- We're slightly more obese, more diabetic, smoke and drink more, than much of the world.
- We have slightly worse vaccination rates (boosters) than the parts of the world where there is widespread access to vaccines (boosters).
- We have minimal mitigation requirements and in many states, bans on mitigation.
I meant to say that we discourage early intervention. ????
Explain the German data.
They're more vaccinated and have free testing.
...but they also aren't taking the same precautions. You see a similar 'southern' problem. They were still doing their nights out and game nights and karaoke (of all things)
Why are they higher at the moment? Because they're still coming down from their Delta wave that peaked at the start of December, with deaths trailing. Once they hit their Omicron wave at peak, they'll look quite a bit different.
Neither our smoking rates nor our alcohol consumption rates are out of sync with peer nations-- a number of which smoke and/or drink more.
Pointing to some comorbidities in some countries does not obviate the fact that all of the comorbidities add up, and we can observe this by the changes in life expectancy of all our cohorts. Here's a handy chart to show this point: https://bityl.co/AZVe
Low Vit D, being too fat.
Here in the US, deaths are closely correlated with age and the likelihood of watching NASCAR races.
When comparing countries, I suspect its the NASCAR doing all the heavy lifting.
US Life Expectancy Vs. # of Taco Bell Locations, Per-State,
https://old.reddit.com/r/dataisbeautiful/comments/s75sm7/oc_us_life_expectancy_vs_of_taco_bell_locations/
Coincidence?
Why is Germany so high actually seems to be a question first, as they in that chart are above USA.
Perhaps the Chinese Communist People's Liberation Army Plandemic Hoax Genocide is a joint op with Neonazis in the former German Democrat Republic to cull the undesirables & boost the odds of AfD seizing power? Axis 2: Electric Boogaloo, when China replaces Japan as Germany's Asian friend.
My instinct is that comorbidites explains most or all of this.
It's generally a confounding variable when US healthcare outcomes are compared to other countries and has a fairly direct impact on how deadly COVID is for an individual, vaxxinated or not.
Should be something that can be controlled for in a study.
I would group the issue into a few factors
First those that affect the actual true ifr, not cfr, for a similar infection. This would include health issues and comorbidities. And also differences in quality medical systems and health care .
I expect that, while there are differences between nations, they are not all that big and I would say this is the smallest factor.
Second , factors that change the types of infections a nation has. This includes the proportion of total cases that are which variant. The higher proportion that is omicron, the lower the total ifr. Nations like Australia which avoided original and delta to a large degree but now are being hit by omicron will have a lower ifr.
Also how many infections are " breakthrough " either from prior infection or vaccination. When the immune system has been prepared at all, death rate is low. Plus, with natural immunity, even if it did not work at all, by definition, breakthrough infections are by definition only in those who already showed they can survive covid. If nation a did nothing and covid infected 100% and killed .5% most vulnerable, and then reinfected in wave 2 killing. 1% of those survivors, their ifr is .3%. If nation b used restrictions to only have one wave of 50% of pop killing. .4%, their ifr is higher but not " worse ".
Third factors related to measurement and counting. The cfr as related to ifr is highly influenced by what % of total infections are confirmed vs. what % of actual covid deaths are found ( which can be over 100% if deaths only " with covid"). This can be greatly changed by testing policy and amount and different criteria on what counts as a covid.
Nations that test extensively and effectively, catching a higher % age of actual infections, but have a more narrow definition of covid death will have a lower cfr even if their actual ifr is the same . And vice versa .
I expect that this factor is the biggest issue in differences between most nations ( not outliers like Australia) and seems to be rarely discusses.
Usa, imo, while having a fairly high testing volume, has an inefficient one in finding cases. Recently, we had many getting tests for school, etc. without any symptoms or knowledge of exposure. While many who were sick could not find a test. Doing that can mean high testing volume but still low % of cases found.
But usa, I understand, has a fairly broad definition of covid death and just about all who die are tested prior at some time ( excepting at start with those dying at home). So we miss few actual covid deaths and have a bit more false covid deaths.
Cosmic justice.
Ours not to reason why, ours but to do and die.