
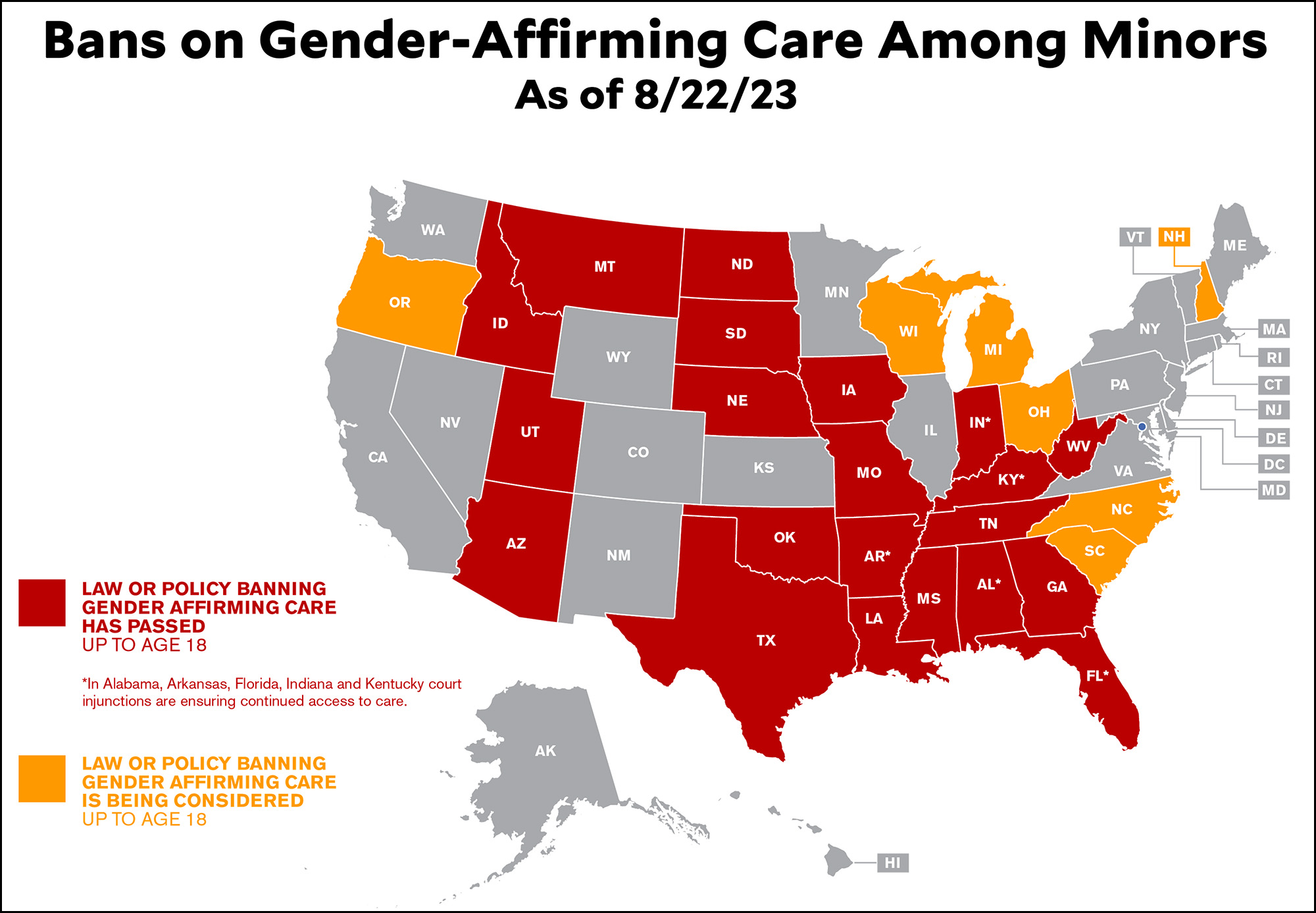
In our Twitter spat a couple of days ago Chris Geidner mentioned a new law that prevented trans kids from getting gender affirming care up through age 18. I corrected that to 17, thinking of the Tennessee law that was recently upheld in federal court. But no. It turns out Alabama has a law that really does go up through age 18, and it too has been recently upheld in court.
But why? The Alabama law talks repeatedly about protecting "minors," who are generally defined as age 0-17. What's the excuse for adding on an extra year?
The answer is that Alabama is one of the few states that defines minors as age 0-18. So at age 18 you still aren't an adult.
But medical care is a big exception. In Alabama, you can get treatment for drugs and alcohol at any age. You can get STD testing at age 12. You can get yourself vaccinated at age 14 (except for COVID). You can get contraceptives at age 14. Or anything else, for that matter:
Any minor who is 14 years of age or older, or has graduated from high school, or is married, or having been married is divorced or is pregnant may give effective consent to any legally authorized medical, dental, health or mental health services for himself or herself, and the consent of no other person shall be necessary.
Now, it isn't unheard of to make exceptions to general age restrictions like this one. Abortion is completely illegal in Alabama, for example, no matter your age. The drinking age is 21, as is the vaping age and the smoking age. You can buy life insurance at age 15 and take out an educational loan at 17. You can't run for governor until you turn 30. The age of consent is 16.
Still and all, the general age of adulthood for medical procedures is 14, and that's without parental consent. Trans care is now basically the only exception even with parental consent, a hysterical submission to the current crusade against trans people from red state Republicans.
 Moral panics like this one generally produce nothing but misery and oppression, and the campaign against gender-affirming care is headed down the same road. It's one thing to display some caution toward procedures that haven't been heavily studied and still have unknown consequences—this is happening in some European countries—but it's quite another to ban them altogether out of bigotry and ignorance. That's what the militant zealots in Alabama are doing, along with their militant zealots in two dozen other states.
Moral panics like this one generally produce nothing but misery and oppression, and the campaign against gender-affirming care is headed down the same road. It's one thing to display some caution toward procedures that haven't been heavily studied and still have unknown consequences—this is happening in some European countries—but it's quite another to ban them altogether out of bigotry and ignorance. That's what the militant zealots in Alabama are doing, along with their militant zealots in two dozen other states.
In the absence of strong evidence in either direction, decisions like these should generally be left up to the patient, their doctor, and their parents. They're the ones best able to make case-by-case judgments. At most, given the current state of our knowledge, states might be justified in mandating a few guardrails (counseling, time restrictions, etc.). But that's it. Banning gender affirming care entirely for minors—the only age at which certain procedures can be done—is nothing more than jumping on the bandwagon of never-ending ugliness that has broken out in the Republican Party in the age of Trump. It's cretinous and disgraceful.
I agree that state legislatures should not be trying to dictate medical care, but I'll point out that currently the bodies who should be taking a look at the current disaster that is pediatric sex trait modification, such as the AAP (American Academy of Pediatrics) AMA, APA have fallen down in their responsibilities.
Now, a couple of weeks ago the AAP announced that they plan to commission a systematic review of the evidence for gender medicalization, and that's good news.
We'll see what happens next.
Over in Europe - Finland, Sweden and England have all done their own systematic reviews of the evidence, found the evidence to be wanting and have characterized this to be experimental, unsupported care. They are backing away from doing medical things to minors in those countries, also in Norway and Denmark. Those countries all have more centralized medical systems and thus they feel a fiduciary responsibility for looking at the evidence base for what they do.
Every single medicine or treatment given to trans children is also given to cis children in much greater numbers. Are we worrying about them?
Doctors have been treating trans people for at least the last 50 years here in the US. But you are sure that you know more than them, or their parents. You've found someone who says it's "experimental".
My daughter is trans. I have met many a trans person and many parents. Not all parents are super-supportive, but all of them, and all of their doctors, take the situation very seriously.
Sometimes things don't go well. However, that's also true of the cis children who get the same treatments, and again, in larger numbers.
Oh, I've found more than someone who calls pediatric medical transition "experimental." I've found whole national health systems, in more than one liberal western country!
It's the combination of GnRH agonists followed by cross-sex hormones and cosmetic/sterilizing surgery that is unique to pediatric sex trait modification. This is a relatively new medical practice, and it's being pursued all over the United States and Canada despite a dearth of solid evidence that it helps more than other strategies for gender dysphoria.
It's part of the unique American medical system that we don't have a national health authority who would be responsible to look at evidence and outcomes. Right now we have "red states and blue states" running in opposite directions on the issue of pediatric gender medicine.
I'm not happy with what's happening on either side. I would prefer a sober look at the evidence. Currently pediatric sex trait modification is not even competing with placebo effect in the papers, suggesting that it might be actively harmful.
For example, Chen et al 2023 NEJM is an NIH funded study that has taken a long time to publish anything. In their application for NIH funding back in 2016, they said they would follow 8 variables including gender dysphoria, depression, anxiety, trauma symptoms, self-injury, suicidality, body esteem, and quality of life.
In the 2023 paper they only report results for depression and anxiety and they report that the most common adverse effect of cross sex hormones was suicidality (wait, I thought treatment was supposed to save kids from suicide). They had two completed suicides in their 315 patient cohort which was screened for suicidality at the outset.
2 suicides in 315 patients is terrible. Often if you have a death six months in to a medical study it leads to a reconsideration of whether what you are doing should be continued.
For comparison, Dr. Michael Biggs over at Oxford did a FOIA request and got suicide data for 15,000 patients referred to the GIDS service at the Tavistock, the world's largest gender clinic. Over a period of 10 years, there were 4 completed suicides. Two occurred in patients who were on the waiting list and two occurred in patients being treated. That is still a suicide rate higher than the background rate for this age group, but it's similar to that for minors diagnosed with things like anxiety, OCD, or depression.
In the original Dutch study, one of the 55 patients died from sepsis following a post-surgical infection related to the use of colon tissue in the vaginoplasty which was required because puberty blocking blocks penile growth and the usual penile inversion technique can not be utilized. And yet, that is the foundation upon which all pediatric gender medicine stands. It's really amazing when you take a look at it.
Chen:
An adverse event does not necessarily correlate with treatment. You should know that. The overall evidence of the study suggests that treatment mediated suicide.
No, you really can't say that "the overall evidence of the study suggests that treatment mediated suicide." I know that's what we want, but that's not what we're getting from this treatment.
The suicide rate amongst study participants - young people pre-screened for suicidality getting treatment at 5 of the best gender clinics in the United States - is something over 50 times the background rate for this cohort normally. One suicide could be a fluke. Two is concerning, to me.
And really, "appearance congruence?" So, if you give ftm's testosterone, they get facial hair and this improves their appearance congruence. OK.
Approximately 40% of _all_ people experiencing GD attempt suicide; at this point I know you know better and are deliberately squirting ink.
Again, suicidality is not the same thing as suicide. I think you're trying to quote the 2015 USTS, although you've got the number wrong even for that.
It's just wrong to claim that sex trait modification is suicide prevention. It most certainly is not.
If you can somehow post the full data set and study, it would be greatly appreciated.
Sorry, I can't.
Why refer over and over to "gender-affirming care"? The word "gender" in ambiguous, and the other words are loaded with (arguably unjustified) positive connotations.
Could you not be accurate and call it "sex trait modification"?
I like that reworking.
Oh, because "gender affirming care" is what the medical community calls it?
But what do they know about it anyway? (Ducks)
It is useful that we all start from "[today's] Republicans are vicious fanatics." They don't care about kids, they don't care about adults, they care about creating fear and loathing.
Kevin -- I really think you need to read some of the critiques of treating Gender Dysphoria (GD) in young people with hormones or hormone blockers (HT). The critiques are relatively straightforward, and point out that the evidence that HT helps young people suffering from GD is pretty much non-existent. Furthermore, the treatments clearly have terrible side effects -- the loss of the ability to have orgasms, and the loss of fertility are common, not to mention the necessity of the patient to stay on hormones for the rest of their lives.
The flaws in the studies showing benefits of HT are glaring and typically include one or more to the following:
* The follow up period is way too short to see if there are problems
* There are *never* any randomly chosen control patients
* The patients' mental health does not improve with treatment
* The studies protocol defines the set of symptoms to be examined, and then only reports on a tiny subset of those
* Significant numbers of non-random people leave the studies and are never followed up
A good summary of the issues was recently written by a psychiatrist on Reddit, but I want to point out that you can read the original papers he references, and see that the statements are valid. Here's a link:
https://www.reddit.com/r/medicine/comments/15hhliu/the_chen_2023_paper_raises_serious_concerns_about/?utm_source=substack&utm_medium=email&rdt=46354
The fact is that the vast majority of youth who suffer from GD but aren't put on puberty blockers stop suffering from Gender Dysphoria on their own, while something like 98% of those put on puberty blockers proceed to cross-sex hormones with irreversible effects ( https://www.thelancet.com/journals/lanchi/article/PIIS2352-4642(22)00254-1/fulltext#%20 ).
In short, the side effects of treatment are undisputed and severe. The treatment doesn't improve the mental health for those treated, and for the vast majority of those who would naturally desist, treatment with HT clearly leaves the patients worse off.
It's for these reasons that the national health services of Norway, Sweden, Finland, the UK and most recently Denmark have all essentially blocked treatment of young people with hormone blockers or cross-sex hormones. France's health department put out an advisory pointing out that there is no good quality evidence supporting hormone treatments for GD, although it stopped short of a ban. Concerns about these treatments is far more widespread than just a few red states.
Now, should this really be left to the parents and competent doctors? Theoretically yes, but clearly American doctors have been led into an affirmative model that's most likely permanently damaging the vast majority of its young patients. Even Planned Parenthood, typically a pretty responsible organization, boasts that if you're over 18 (some chapters it's over 16 with parental consent) you'll be prescribed cross-sex hormones on your first visit. So, it's not completely irrational for some states to just ban these procedures for minors.
Every treatment given to trans children is also given to cis children, in much larger numbers.
Funnily enough, you aren't trying to protect all those cis children from those treatments, are you?
We're not sterilizing cis children in response to emotional distress.
If you are doing extraordinary treatments (and treatments with these levels of morbidity and mortality are extraordinary) you need extraordinary evidence to justify what you are doing. We can't even agree on how to diagnose these kids.
America's first pediatric gender clinic opened in 2007, that's less than 20 years ago. This is an innovative medical practice that escaped the lab and became widely used before it was well tested.
It's time to change the color for North Carolina to red.
I think Kevin, who most of the time strikes me as moderate in a good way, might be suffering from a bit of a “Fox News Effect.” I’m not talking about the Fox News Effect that motivates comically uninformed radicals to invade the Capitol building, I’m talking instead about the tendency among Liberals to distrust or dismiss anything that conservatives support.
Perhaps the first and most obvious question to ask, one that brings a wrecking ball to the thesis of this entire blog post, is why one European country after another has pulled back on gender care and imposed more regulations on gender-related medical procedures. Are all of those countries, to borrow the terminology with which this blog post describes certain Republican state legislators, “vicious fanatics”?
Obviously , Kevin is a smart guy, and he’s aware of this problem, so he states: “It's one thing to display some caution toward procedures that haven't been heavily studied and still have unknown consequences—this is happening in some European countries—but it's quite another to ban them altogether out of bigotry and ignorance.”
But I feel that this statement basically contains its own counter argument. I applaud the honesty which recognizes the fact that some gender affirming procedures “haven't been heavily studied and still have unknown consequences.” But, once that admission is made, logic would seem to direct us more in the Republican direction than we may like. Because, when dealing with a lack of evidence and a host of unknown consequences, especially in any situation relating to children, basic decency if not plain old common sense demands that we proceed with a hell of a lot more than “some caution.” No, we need to proceed with extreme caution, and the only way we could come to a different conclusion is if we’ve got a pair of ideological blinders on.
And then there are statements that I just disagree with: “In the absence of strong evidence in either direction, decisions like these should generally be left up to the patient, their doctor, and their parents.” Let me say right up front that, while certainly experiencing my fair share of illness, I’ve been fortunate in that I’ve never had to undergo any sort of major or prolonged medical treatment. So, my sincere sympathy lies with anyone who has had to do so. Nevertheless, I will proceed to assert that I don’t see the logic of Kevin’s statement. Perhaps, and I hesitate to overstep here, he may be reflecting on his own cancer care; but, call me whatever vile term you want, I don’t think the imminent death that some cancer patients face without a powerful and possibly untested medical intervention can be reasonably compared to the situation faced by trans individuals. In the case of trans individuals, therefore, I think an entirely reasonable argument can be made for stronger regulation of the care they receive.
But that brings us to the main point, how much regulation is the correct amount? Again, I disagree with Kevin’s assessment: “At most, given the current state of our knowledge, states might be justified in mandating a few guardrails (counseling, time restrictions, etc.).” Well, Kevin has already admitted above that the “current state of our knowledge” is limited, and it would strike me as clearly obvious that, in that case, we should therefore adopt a MORE careful approach rather than a less careful approach.
But does that conclusion therefore lead us to endorse the Republican state bans on gender affirming care? I don’t know. Taking Kevin’s own concessions into consideration, and acknowledging that our knowledge is limited, I’m inclined to think that a ban is a more prudent approach (at this time) than the generally permissive approach that Kevin inexplicably promotes.
But I’ll certainly acknowledge that it’s a hard call. And you know what doesn’t help us resolve the issue? Assuming that anyone who disagrees is an evil bigot. And that’s where Kevin sadly takes a wrong turn deep into the Fox News Effect when he says, “Banning gender affirming care entirely for minors—the only age at which certain procedures can be done—is nothing more than jumping on the bandwagon of callous ugliness that has broken out in the Republican Party in the age of Trump.”
Trump has done so much to derange not just republicans but also Democrats, and that statement from kevin is a good example of the derangement I’m talking about. It infects otherwise good blog posts like this one and leads them into utterly unnecessary character assaults on some of our fellow human beings.
Speaking for myself, I certainly hold both far right as well as far left extremists in suspicion, but I try to avoid claims that I can read their mind or hearts. I still mess up sometimes. We all do. But we need to be more careful. This issue will not be resolved by further inflaming culture wars. If we go down that path, we will almost certainly wind up harming the very people we ostensibly want to help.
And yet, there is a difference between a blanket ban and stronger regulation, and KD's post is highlighting the spread of blanket bans.
Should states be allowed to ban sugary drinks, or should they regulate them by proxy using a structure of "sin taxes"?
1) why is a ban ‘more prudent’? Persons with gender dysphoria are known to be at higher risk for mental illness and suicide. It’s not irrational to want to do something to ameliorate those risks. Perhaps current treatments does not significantly reduce those risks, perhaps it does; one hopes there will soon be better data on the issue. Both action and inaction carry some risk; neither alternative is obviously ‘more prudent’.
2) until we have better data, why do some commenters here think that state legislatures are better able to weigh the risks and potential for improvement better than medical professionals?
It's all about the suicide, because death is the only feared outcome that can justify destroying the sexual function of children. Marci Bowers MD, president of WPATH and Jazz Jenning's surgeon, is on record stating that "pretty much every" male child put on puberty blockers at the onset of puberty has been anorgasmic for evermore.
There is no evidence that pediatric sex trait modification decreases the numbers of deaths by suicide. In fact, evidence is growing that it may make things worse.
Re-read my point 2).
Oh, at this point, I think we all know that he knows better. He's sea-lioning.
Re-read my comment at the top of this thread! I don't think state legislatures should be trying to regulate medical practice.
Let us not even begin to pretend that concern for the health and well-being of kids has anything to do with Republican motivations in passing these laws.
Does cis breast augmentation/reduction fall in the same category as these treatments? Why or why not?
Me, I think it's extremely tough to fit the general to the specific, even in good faith. Plus, it's none of my damn business what other people get up to with their own bodies, and say, itsn't that supposed to be a libertarian -- and hence Conservative -- thing?
Well, breast reduction/augmentation surgery doesn't typically leave you unable to orgasm or be a biological parent. It's probably near reversible. It doesn't require a lifetime of hormone treatments.
Inability to orgasm, lifelong meds, tell me then why it's okay to administer antidepressants to pre-adults? Unless you're saying unable to have kids is the dealbreaker?[1] And you forgot to mention that breast augmentation can give you cancer.
[1] I don't know whether you're being deliberately obtuse or just don't get it: Why is tihis particular protocol _quatitatively_ different? Because there are any of a number of medical procedures that can do the same thing ... or worse,
The irreversible part, which I mentioned in my response, combined with the inability to orgasm or have children, makes it significantly different from your examples.
On top of that, of course, is the likelihood that the effectiveness of the treatment is being misrepresented. That's what all those European health departments are saying -- the treatment doesn't actually reduce GD distress, and has all these negative side-effects.
[I don't know why you're accusing me of being deliberately obtuse. These treatments are essentially irreversible, require a lifetime of medication whose side-effects over decades is unknown, and have major side-effects. There's no way that a 12 year old considering starting these treatments can provide informed consent to all of that.
This is nothing like a breast implant that can always be removed.]
"The irreversible part, which I mentioned in my response, combined with the inability to orgasm"
You don't know much about antidepressants, do you:
I find it hard to believe you don't know what is common knowledge about antidepressants, ergo, you're just cutting and pasting talking points. Care to admit you were wrong? If not, why should I take you seriously?
Classic obtuseness and, borrowing from another comment of yours, picking your facts only b/c you like them.
SSRI have these effects largely WHILE TAKING THEM. There are reported instances of long-term dysfunction, but given the huge numbers of people taking SSRIs all sorts of odd effects should be expected. Have sexual dysfunction? Stop and most people recover.
Kids on puberty blockers go through distinct development periods without actually developing. There's no going back.
And SSRIs are actually approved for the use of treating depression. Puberty blockers are not FDA approved for treating gender dysphoria.
So yeah, they're not comparable.
Again, echoing what GrumpPDXDad says, ****irreversible**** inability to orgasm. ****Irreversible**** loss of fertility.
The very first sentence in my earlier reply mentions the irreversibility of these cross-sex hormones. This time I've emphasized by surrounding the words with asterisks why cross-sex hormones differ from SSRIs, which, BTW, are not the only anti-depressants on the market.
But you just said, oh forget it. You know that you have to take antidepressants all your life. It doesn't go away. Yes, I know people who've forgone anything to do with sexual enjoyment for a life where they can at least get out of bed. And they've done it for decades.
It occurs to me that you don't have any idea of which way the burden of proof flows here, which is from you to me, and that is because of the singular nature of these draconian laws. Which is to say you've got to prove to my satisfaction that these laws exist for good reason, not the other way around.
You've also, needless to say, have to be consistent in the application in your reasoning; you have -- also needless to say -- not been consistent, as I've just shown be example. You'd have done better not adopt a scattershot approach and concentrated on one point. Me, I'd have gone for irreversability ... but not before researching other medical procedures that are also irreversible.
I'm sorry if anyone told you that you have to take antidepressants for the rest of your life. I do write Rx's for SSRIs and I've always viewed them as a temporary salve, something to turn the volume down on all the things stressing my patient excessively.
They are a tool to create space for healing, which is primarily derived via good therapy. Every spring I suggest decreasing the dose or discontinuing the medication.
You're in no position to dispense script you goddamn liar. Oherwise you would _know_ that lifetime meds are the norm.
Nice shot trying to imply that I'm on meds myself; you're showing your hand.
I'm a pediatrician and no, lifetime meds are NOT the norm.
Gee. I'm old enough (ie older than 30) to remember when the Left was thoroughly AGAINST breast surgery for teenagers and would loudly mock this as some combination of
- the "patriarchy" imposing its will on innocent children, and
- the hillbilly choices of benighted southerners...
Have we switched to always being at war with EastAsia? Are we now supposed to demand free bigger/smaller tits with your Quinceanera as a right implicit in the Constitution?
Well I’m being educated here in the comments, hopefully so is KD. Based on what he posted, it would appear he does not think gay conversion therapy should be made illegal. Here is the thing, when it come to minors we all should thread very carefully and we should recognize that parents and doctors can make bad decisions, and in this instance, a bad decision is for life. I can see why people ask where the state was when others ruined their lives, IOW, the state has a very strong compelling interest in the manner.
The state has a very strong compelling interest in preventing the religious brainwashing of children by their parents. The state has a very strong compelling interest in ensuring children aren't poorly and noxiously educated by parents who have an ideological axe to grind. Now which causes more damage? The two I mentioned (I could name many more)? Or the one you're on about?
Priorities.
Even if parents + doctors + patients are all wrong once in a while, that hardly seems to be a solid basis for the state to place a blanket ban.
If multiple people make poor judgments with regards to alcohol resulting in the deaths of others, should the state therefore ban all alcohol?
The comments of drfood4 and PittsburgMike and Leo1008 are thoughtful contributions that get at some of the essential difficulties in this area. But it may be worth digging deeper, to ask what is the point of "pediatric sex trait modification"?
The intuition that has captured so many people is that a child can have an "innate gender identity" that differs from his or her sex. Thus for instance a male in the ordinary sense may in reality be a female in some more fundamental or essential sense. In fact, this seems almost obvious once you say that "she is a trans female". The term "trans female" confers a kind of ontological status. The "pediatric sex trait modification" is then intended to converts body features to align with the deeper reality.
The problem with this is that it is a metaphysical view much akin to views in which one talks of the "soul of the fetus". In other words, this "deeper reality" is mysticism. There is no evidence for this view, and it is even difficult to make it coherent. (Can one have an internal feeling of one's sex? How would you know you got it right? Just because you prefer dolls to trucks?)
But can't you approach this without mysticism? Of course. Take for instance a female who is convinced that all along she has been a male. Say that, although this is false, her conviction is so strong that her feeling of non-alignment causes deeps distress.
But then "pediatric sex trait modification" seems less pressing. What else could be going on? Does this female have a brain that somehow gives misleading signals? Does she have psychological issues for which she has found a mistaken solution? Did she spend too much time on the internet? Whatever the reason, it is not that she is "really" a male. To justify "pediatric sex trait modification", one should surely explore other reasons first, and even then one has the difficult task of predicting what will make her outcome positive over a period that may include many decades of adult life.
It used to be thought that homosexuals were bon wrong (apologies for the deliberately archaic phrasing); do you still think that is the case?
Interesting points. The NHS in England asked Dr. Hilary Cass to look into the field of pediatric gender medicine. She wisely said that there are many paths into gender dysphoria, and also many paths out.
Sex trait modification should be reserved for those who are unable to manage their gender dysphoria by other means. In the before times it was noted that 66-88% of young kids who expressed a desire to "change sex" had a natural desistance with the onset of puberty, and most of these kids turned out to be gay. With puberty (if it is allowed to happen) a person has their sexual awakening and this can help a kid make sense of why they felt different from the other boys or girls.
This strategy was the standard of care in most of America prior to 2015 and was called "watchful waiting." You supported the child in their preferences, but didn't tell them that they were "born in the wrong body."
I think that map is wrong. Oregon has no such bill under consideration that bans gender-affirming care below 18 years old. How would that happen? The legislature is fully controlled by Democrats and the existing law allows 15 year olds to receive gender-affirming care w/o parental consent.
Ditto Michigan. Someone in the GOP nut caucus in the House may be pushing a bill but the Dem majority will ignore it, Whitmer will veto it and the Dem majority in the Michigan Supreme Court will rule it unconstitutional.
Your mapmaker needs to take into account which bills are viable and which bills are for Buncombe.
https://www.ncpedia.org/buncombe
"In the absence of strong evidence in either direction, decisions like these should generally be left up to the patient, their doctor, and their parents. ..."
If some religious cult such as the Branch Davidians were doing things like this to children against the wishes of their parents in order to say cast out demons I expect Drum would be horrified. But put some pseudo-scientific veneer on it and suddenly Drum is deferential.
Really putting your thumb on the scales there arent ya? With no actual argument or counterargument, the best approach is clearly to try to cram as many logical fallacies into your comment as possible.
Allowing women and their Dr to decide on the womans medical care is just like allowing rapists to determine medical care for the woman they raped! ITS THE SAME THING AND YOU ARE A MONSTER!
Lol, internet comments are the best.
Your example doesn't seem analogous.
In your example, parental opinion is rejected, regardless of a child's wishes to have their demons cast out.
In the case of trans youth below a certain age, parental approval is required.
"In the case of trans youth below a certain age, parental approval is required. "
And Drum suggests that age should be 14. So minor children. And I doubt Drum thinks parental approval is sufficient for similarly drastic "treatment" of demonic possession.
The number of older people creeped out by this and making emotional arguments disguised with pseudo-sciency sounding claims certainly sounds a lot like the bigotry around gay and black Americans. Lots of emotional and 'sciency' sounding reasons to deny these people the ability to lead full lives.
Each time, the zealots insist that their zealotry is nothing like the crazies that came before (after all, they have a black friend)....but, its not very convincing.
While I think you are right that there is a fair amount of discomfort and bigotry regarding trans people right now, that does not tell the whole story. Gay and black children don't need medical intervention to complete the process of being gay or black, so this is a little different.
Personally I'm inclined to Kevin's point of view, that people should generally defer to the parents, kids, and doctors in these situations, and I'm 100% against the state stepping in the middle of these decisions.
I do think our culture has too much of an obsession with body modification in general and feel that all people (trans, non-trans, etc.) would be better off learning to love and appreciate the body that nature gave them and not expecting medical science to give them the body they wish they had (whether it's one with big boobs, a firmer butt, fewer wrinkles, or different gender characteristics). Maybe that makes me an old man or a prude. But I think we are all generally better off if we minimize the number of drugs we take and the number of surgical procedures we receive. You can live as a woman or a man without necessarily having medical science step in.
Think about how our society treats overweight people. Often very badly for sure. But we don't have an expectation that all overweight people should immediately seek out liposuction and lap band surgery to be thin conforming, as it were. OK in a way we do, but this is not something anyone thinks we actually should do. The phrase "fat shaming" exists for a reason. We try to counsel self acceptance, and acceptance by others when it comes to the overweight. I'm not sure why this kind of self acceptance movement can't make its way into the trans community. Why should society's expectations of the outward manifestations of masculinity and femininity be such primary considerations when it comes to how we deal with trans people?
But that's just, like, my opinion man. I would not support any sort of state intervention to prevent people from doing what they choose to do.
" I would not support any sort of state intervention to prevent people from doing what they choose to do."
You mean you're -- Gasp! -- a Conservative!?!?!?! Whoda thunk? I likes me being an Eisenhower Republican, not the least because it's more consistent than a lot of political identities to the right of it.
Again, this is garbage. It is blatantly discriminatory.
Every single treatment that falls under the rubric of "gender-affirming care" is given to cis minors in much higher numbers than it is given to trans children.
Did you know that there are 3000 or so top surgeries given to cis women under 18 per year? That hormone blockers are routinely used to combat early onset of puberty? That HRT is used to deal with other problems?
Nobody says doctors are falling down on the job with regard to these children.
No, what's going on is discomfort with the existence of trans children. People want to be rid of them, and don't trust their parents, or their doctors.
I for one think breast surgery to a cis teen is a crazy idea, one I would never endorse. But I'm not advocating for laws that prevent it.
I fucking hate this bothsiderism here: "Well, we maybe shouldn't have laws, but the thing I'm REALLY concerned about is that there's too many trans kids".
I hear you Dr. Jay. I know, what seven? Eight? Anyway, a fair number of -- I would say kids, but the eldest is close-on thirty now -- who transitioned, all of them successfully. Furthermore, I knew them some time before transitioning; each and every one of them are much happier after than ever they were before. I know, I know, anecdata, but the statistics back my idiosyncratic experience as well. How many trans people do the likes of drfood4, PittsburgMike, Leo1008 know? (I deliberately left out low grade troll GrumpyPDXDad who argues like they took a few too many shots to the head; not fair to pound on them too hard.)
"women under 18"
Trans or not, "women" under the age of 18 are properly called "girls".
My daughter informs me that this is most emphatically not the case.
Check out one woman's story, courtesy the best paper in my hometown. Yes, I know Karen personally.
The ick factor coming from some commentors is obvious and quite strong. Let's posit a Chip Delany future where sex changes are safe, routine, and above all, easily and repeatedly reversible, cf. Triton. Would these worthies have still be throwing everything but the kitchen sink into their arguments for banning trans procedures?
Kevin, I would like it if you would do one of your deep data dives and then make a chart or two like you like to do. I would like you to compare the number of cis children treated with the same medication and/or procedures as are being banned for trans children. I would like you to make a chart. I would like to hear your reaction.
If you want to consider side effects or unintended outcomes of these treatments, then compare them, too cis to trans. I think it would be interesting.
I was upset with your post yesterday because you didn't do these things before offering "they may have a point" with regard to care. They don't have a point. It's bigotry and discrimination all the way down.
"Moral panics like this one generally produce nothing but misery and oppression, and the campaign against gender-affirming care is headed down the same road."
Probably true BUT...
Exactly what is the theory of human nature that claims say 15 year old is capable of knowing themselves and their body enough to go down the trans path, but a 21 year old is NOT capable of knowing themselves and their body enough to be always be responsible for consensual sex?
The TERF side of this debate is basically honest – they claim that kids don't know what they want, about pretty much anything, and that's why it's reasonable to constrain their choices. But the woke side of this debate seems to want to have it both ways, insisting that for some purposes anyone, even a 6 yr old, is capable of making informed choices whereas for other purposes pretty much everyone, whether a 21 yr old student or a 45 yr old undergoing a medical procedure, is incapable of informed consent if claiming such will punish someone of a non-approved class.
There are some good comments on here, but also a lot of intellectually dishonest ones. It is disappointing to me.
As a father of two trans children, I have had to learn a lot in a relatively short period of time. I haven’t spent as much time on the scientific literature as on the records of trans people’s lived experience. Both of my kids are over 20, the older one is on hormone therapy and had breast reduction surgery this summer. He is so much happier and more balanced that I find it incredibly easy to adapt to the change. The younger has only tried binders so far. That situation is different for a whole host of other reasons, but we have encouraged him to seek his own path while gathering as much information as possible.
To my mind, blanket bans are simply stupid. They tend to be based on little or no evidence and are widely supported by publicly bigoted people. It is hard to look at the most recent red state actions and see any real concern for the wellbeing of children.
The pullback in various European countries appears to be much more based in a somewhat unbalanced concern about what evidence exists, but is much more informed than what I see in the US.
I really appreciate Doctor Jay’s insistence on including evidence for HRT from the experience of cis kids and adults. Until one looks at the whole universe of evidence, one cannot make a useful policy statement.
In any case, I am in favor of letting people find their own way through life as much as possible while doing everything we can to reduce harm of all sorts.
I'd say it's not an unbalanced concern as much as a lack of terribly relevant data.
There is growing evidence in right wing hell hole countries like Denmark, Sweden and Norway that most kids don't need gender affirming care, as pueberty resolves many of the issues. That is the growing scientific evidence. Puberty blockers also have some downsides and may not be appropriate either.
But the point is you are right: each case is largely individualized and what is appropriate for some is not a good fit for others. And a patient and medical professionals should be able to determine what care is needed without things like a ban. A patient should always have the option to get the care they need.
We should take seriously anyone of any age who is living anywhere on the gender dysphoria spectrum, and if medical attention is called for, they should get it. I'll leave it to smarter people than I to figure out when or if medical attention is called for.
But whatever rationales these red states can dig up for their bans, they are not, I believe, really based on medical science or genuine interest in anyone's welfare, but on some weird combo of religious pretense, ick factors and just plain hatred. On that basis alone I'd do away with the bans if I could. And no, I don't have to prove the hypocrisy behind bans on gender affirming care, or same-sex marriage, or abortion.
At this point it's necessary to say that 'drfood4' is deliberately misrepresenting himself as a medical authority. Dude, you just made my shitlist.
Oh no, whatever will I do?
Get back to seeing patients, I think.
I'm not going to worry about the opinion of a rando in a comments section.